Article Text

Statistics from Altmetric.com
Description
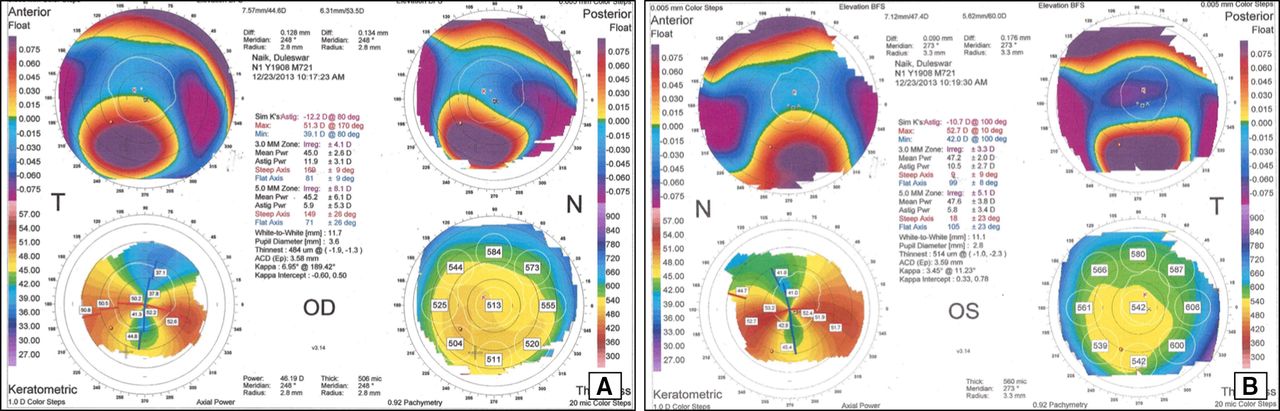
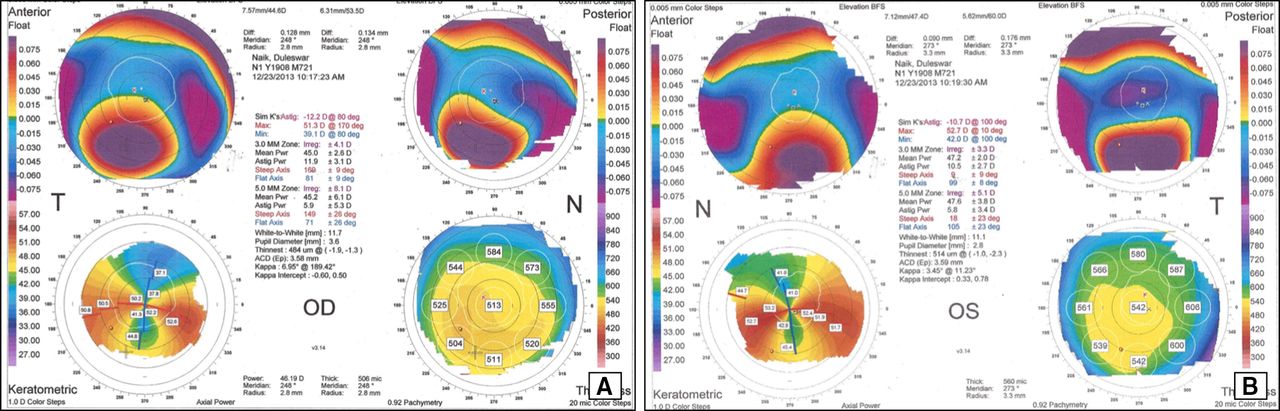
A 54-years-old man, a known case of oculocutaneous albinism (OCA) type 1, presented to us with gradual-onset diminution of vision both eyes (OU) for 5 years. The patient had no prior history of ocular trauma. There was no history of any systemic illness, especially collagen vascular disorder. The best-corrected visual acuity (BCVA) was counting fingers 1 m and 2 m, with refraction of −13DS/−2 DC @ 110 and −14 DS in right (OD) and left eye (OS), respectively. Ocular examination revealed bilateral horizontal, jerky pendular nystagmus of moderate amplitude and frequency, with null at straight gaze. Slit-lamp examination revealed bilateral inferior band of corneal steeping with ectasia, hypopigmented iris with transillumination defects and cataractous lens (figure 1A,B). Dilated fundus evaluation revealed hypopigmented fundus with prominent choroidal vessels and blunted foveal reflex OU (figure 1C,D). OU Orbscan (Bausch and Lomb) revealed against the rule astigmatism, inferior corneal steeping (anterior–posterior float), ‘crab-claw’ pattern (keratometric map) and inferior corneal thinning from 6 to 8 o’clock (figure 2A,B). Based on above findings, a diagnosis of OU pellucid marginal degeneration (PMCD) with OCA was made, was advised for cataract extraction along with intraocular lens implantation. His BCVA improved to 20/80 and 20/60 in OD and OS, respectively, and has remained stable at the last follow-up visit.

Slit-lamp picture of both eyes (A, B) shows inferior corneal ectasia. Fundus photograph of both eyes (C, D) shows dull foveal reflex and hypopigmented fundus with prominent choroidal vessels.
{kind=link}
{kind=link}
Orbscan of both eyes (A, B) shows flattening of cornea in the vertical meridian, against the rule astigmatism, 3 mm and 5 mm zone difference outside normal limits (>1.5 D and >2 D, respectively), steeping in inferior part of cornea on both anterior and posterior float, crab claw appearance on keratometric map and thinnest pachymetry in inferior part of cornea (from 6 to 8 O’ clock). OD, right eye; OS, left eye.
OCA is an autosomal recessive disorder of generalised hypopigmentation, with OCA I being the most severe form.1 Various ocular manifestations of OCA include photophobia, pendular jerky nystagmus, iris transillumination defects, foveal hypoplasia, abnormal decussation of optic nerve head fibres and strabismus.2 Though coexistence of OCA and keratoconus has been stated earlier3; to our knowledge the association between OCA and PMCD has never been reported in the literature. Prior studies in mice strains have documented the strong association of corneal thickness with skin pigmentation, therefore, corneal ectatic disorders in the setting of OCA are more likely a consequence rather than independent association.4 PMCD is a rare bilateral ectatic corneal disorder, involving inferior 4–8 o’ clock in most of the cases, commonly discovered between 2nd and 5th decade.5 6 Hallmark of PMCD on topography is zone of corneal thinning with obvious flattening of the cornea along the vertical meridian and ‘against-the-rule’ astigmatism. Characteristically ‘crab-claw’, ‘butterfly’ or ‘kissing doves’ in topography map also points towards PMCD, though not conclusively.7 The incumbent case highlights the unusual and extremely rare coexistence of bilateral PMCD with OCA.
Patient’s perspective
I am happy that my disease could be diagnosed at an early stage so as to be on routine follow-up and prevent future complications. I and my family members have been apprised about my condition, its natural course and possible complications.
Learning points
Oculocutaneous albinism (OCA) can rarely be associated with pellucid marginal degeneration.
Corneal ectatic disorders in the setting of OCA are more likely a consequence rather than independent association.
Ethics statements
Footnotes
Contributors AK and KA: data collection, writing manuscript. SKP and SKS: reviewing and conception of idea.
Funding This study was funded by Hyderabad Eye Research Foundation (LVPEI-243640-2021).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.