Article Text

Statistics from Altmetric.com
Description
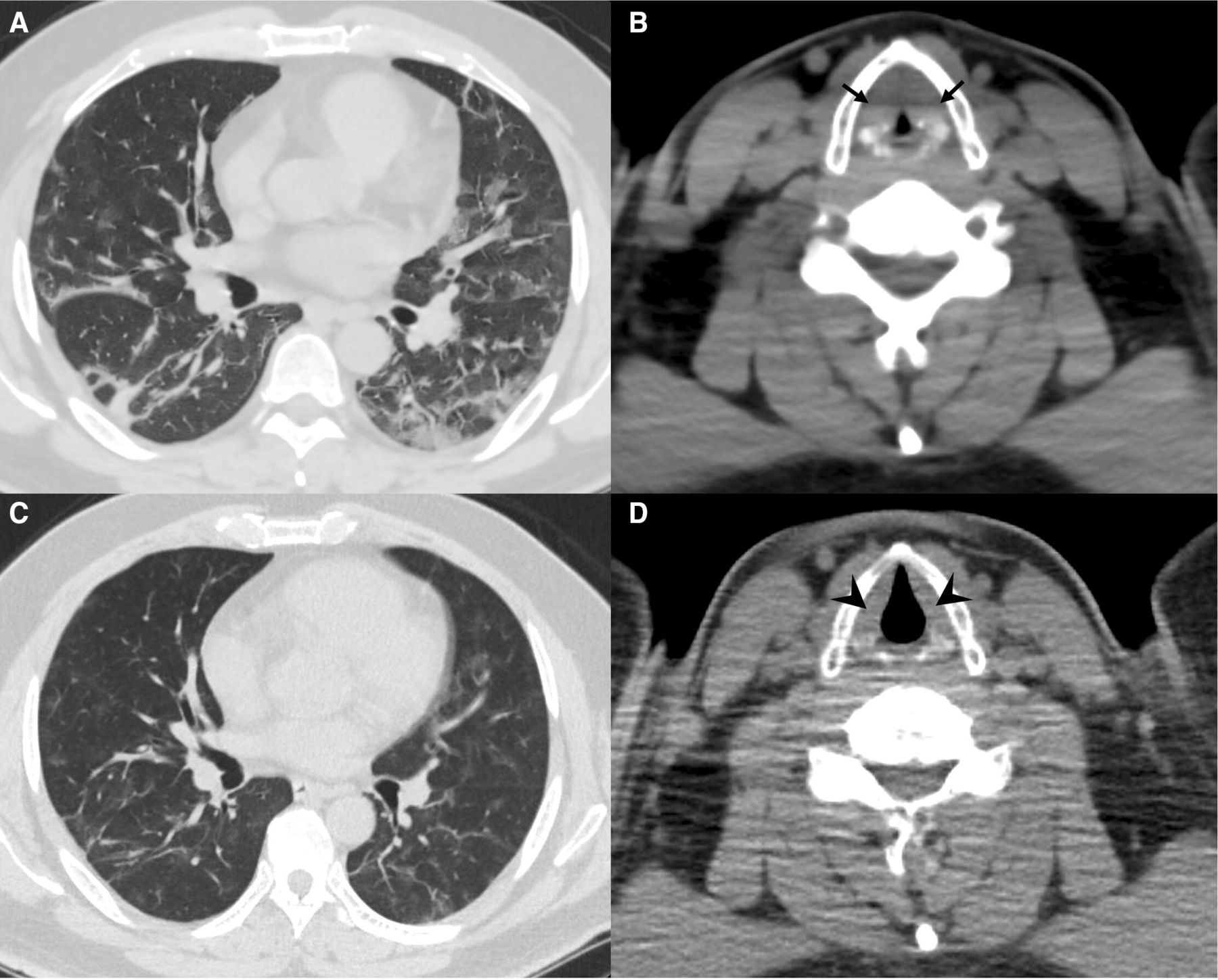
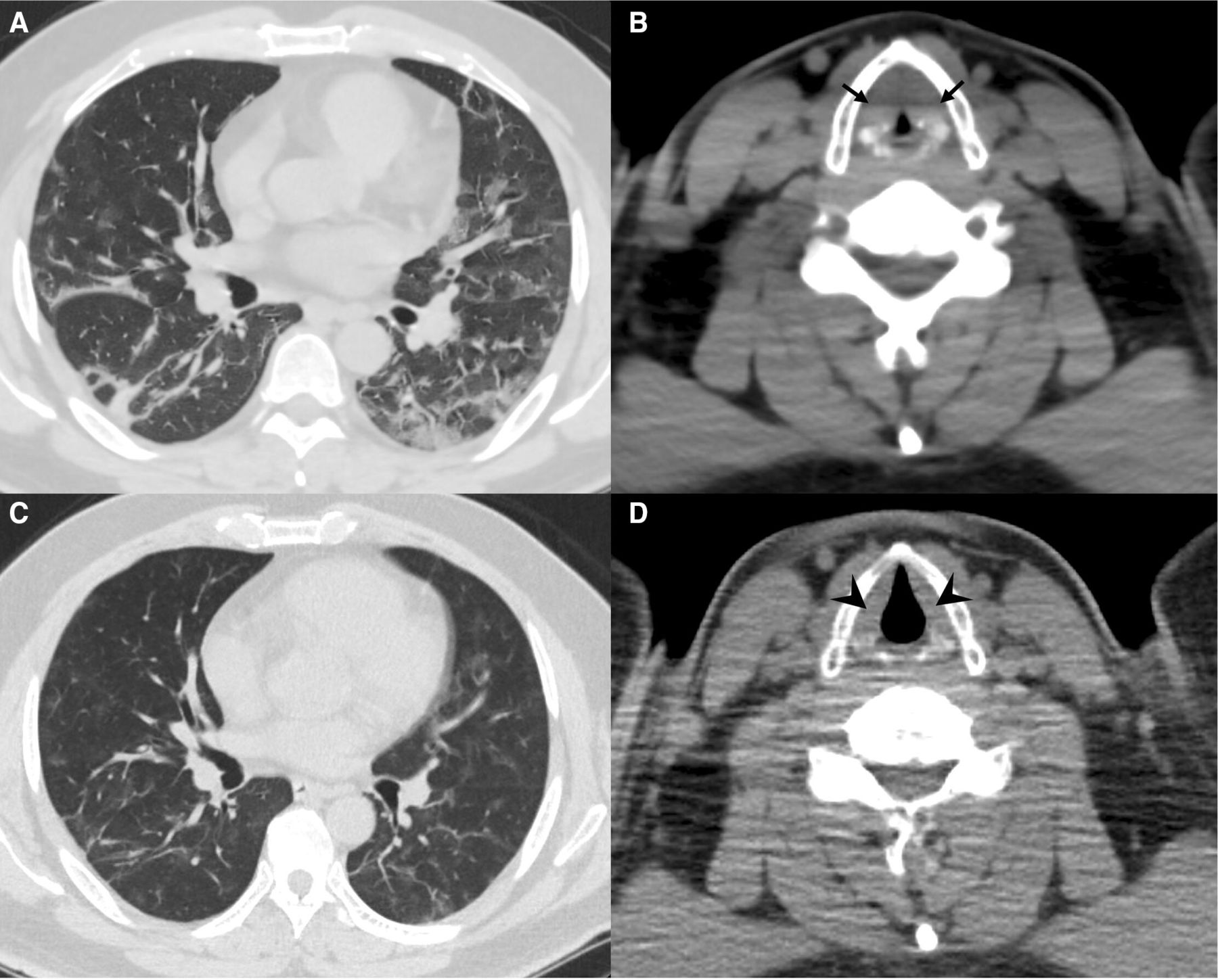
A 44-year-old man with obesity, but no other comorbidities, presented with a 3-day onsets of fever and headache. On examination, he was not in respiratory distress, his body temperature was 38.0°C, body mass index was 35.8 kg/m2 and oxyhaemoglobin saturation was 98% on room air. Novel COVID-19 was confirmed on nasopharyngeal swab PCR testing, and he was admitted to our hospital. On day 5 of admission (8 days after symptom onset), he experienced rapidly progressing acute hypoxemic respiratory failure and was treated with dexamethasone (6.6 mg intravenously) and remdesivir (200 mg loading dose intravenously on day 1, followed by 100 mg/day for 4 days). On day 7 of admission, he reported of new-onset hoarseness and difficulty breathing at rest. CT revealed bilateral peripheral/basal-predominant ground-glass opacities with linear opacities and laryngeal oedema (figure 1A,B). His symptoms were considered to be due to laryngeal oedema rather than pneumonia, and he was treated with a hydrocortisone drip (100 mg). On the next day, his symptoms became less severe, and dexamethasone (6.6 mg intravenously) administration was continued for 10 days. On day 14 of admission, all his symptoms were completely improved, and follow-up CT revealed an improvement of both lung involvement and laryngeal oedema (figure 1C,D). On day 19 of admission, the patient was discharged.
{kind=link}
(A) Chest CT image on day 7 of admission showing bilateral peripheral/basal-predominant ground-glass opacities with linear opacities. (B) Neck CT images on day 7 of admission showing bilateral laryngeal oedema (arrows). (C) Chest CT images on day 14 of admission showing improvement in COVID-19 pneumonia. (D) Neck CT images on day 14 of admission showing improvement in laryngeal oedema (arrowheads).
Discussion
We report a rare case of COVID-19 infection with laryngeal involvement. Our main findings are as follows: first, laryngeal oedema may be a critical complication of COVID-19 infection, and CT can be an alternative to laryngeal fiberscopy for the detection of laryngeal oedema. Second, systemic steroids may be effective against not only COVID-19 pneumonia but also the associated laryngeal oedema. Laryngeal oedema is an acute inflammation of the larynx that presents with difficulty breathing, hoarseness and stridor. Although most patients with COVID-19 experience upper airway symptoms, laryngeal oedema should be considered because it may cause sudden obstruction of the upper airway requiring rapid airway management. It is mainly caused by bacterial infection, injury from smoke and heat inhalation and as a complication of intubation.1 2 There have been several case reports of laryngeal oedema in COVID-19.3 However, all patients were diagnosed with postextubation laryngeal oedema. Our patient did not receive any intervention that could have caused laryngeal injury, such as intubation or suctioning. In addition, he had no smoking history or evidence of bacterial infection. Consequently, we considered that severe acute respiratory syndrome coronavirus 2 directly infected the larynx. As the mechanism of laryngeal involvement in COVID-19 is unclear, further studies are warranted.
In conclusion, we encountered a unique case of COVID-19 infection with laryngeal involvement. In this case, laryngeal involvement developed 7 days after hospitalisation. This case highlights that COVID-19 infection may cause life-threatening upper airway symptoms.
Learning points
laryngeal oedema may be a critical complication of COVID-19 infection, and CT can be an alternative to laryngeal fiberscopy for the detection of laryngeal oedema.
Systemic steroids may be effective against not only COVID-19 pneumonia but also the associated laryngeal oedema.
Ethics statements
Patient consent for publication
Footnotes
Contributors MA and SC attended to the patient, and MA and SC wrote the manuscript. YY and KF reviewed and approved the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.