Article Text

Abstract
Intravascular large B-cell lymphoma (IVLBCL) is an aggressive and rare type of diffuse extranodal B-cell lymphoma. Diagnosis and treatment are challenging and clinical presentation is variable. Physicians should be aware of this rare but life-threatening lymphoma without adenopathy and treatment should be promptly started. We describe the case of a 70-year-old woman who presented with general malaise, acute dyspnoea, platypnoea and lactic acidosis. Echocardiography revealed an extracardiac shunt, the cause of her orthodeoxia. The patient developed rapid liver failure and underwent liver biopsy. Anatomopathological findings suggested IVLBCL, non-germinal center type. She achieved complete remission after rituximab, cyclophosphamide, doxorubicin, vincristine, methylprednisolone chemotherapy but relapsed 1 year after initial presentation with multiple organ involvement. The patient’s relapsed disease was treated with rituximab, iphosphamide, carboplatin, etoposide and she is still in complete remission 2 years later.
- haematology (incl blood transfusion)
- respiratory medicine
- malignant and benign haematology
- liver disease
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- haematology (incl blood transfusion)
- respiratory medicine
- malignant and benign haematology
- liver disease
Background
Intravascular large B-cell lymphoma (IVLBCL) is a rare but aggressive non-Hodgkin’s lymphoma characterised by the presence of neoplastic cells in the lumen of small and intermediate blood vessels.1 2 As IVLBCL is a rare entity, few large series are available. The main series in the literature describe a wide variety of clinical presentations that have been historically grouped into a ‘Western’ variant, characterised mainly by cutaneous and neurological involvement, and an ‘Asian’ variant in which more organs are affected.3 Recently, a new classification of three clinical types with different prognoses has been proposed: a cutaneous form with better prognosis, a form that is associated with haemophagocytic syndrome (HS) and carries the worst prognosis, and a ‘classical’ form that involves multiple organ involvement without HS, and has variable severity.4 Although some series have suggested that, in the rituximab era, the overall prognosis for IVLBCL may approach that of other diffuse large B-cell lymphomas, the disease is commonly diagnosed at stage IV and has a high International Prognosis Index, reflecting poor prognosis.5 6 Moreover, the extranodal and variable clinical presentation of IVLBCL makes diagnosis harder. Therefore, awareness of the disease and knowledge of clinical or biological signs that might bring the diagnosis to mind are essential to starting treatment in time. This patient case illustrates presentation of an acute course of IVLBCL with multiple organ involvement and some specific features that are worth remembering.
Case presentation
This patient was a 70-year-old Caucasian woman without any relevant past medical history. She was on vacation abroad in Europe and had been travelling in Africa 2 months before admission. She presented herself at the emergency department with general malaise, epigastric and upper right abdominal pain, palpitations, dyspnoea, and a slight fever for the past few days. She had been prescribed levofloxacin for suspected pneumonia without any improvement. She had experienced a self-resolved episode of diarrhoea a few weeks before. Vital signs at admission were as follows: blood pressure 115/80 mm Hg, pulse oximetry 95%, cardiac pulse 95 per minute, temperature 36.3°C. Physical examination revealed slight dehydration, tachypnoea without respiratory distress, platypnoea and a painful abdomen with normal sounds, mostly epigastric and right hypochondrium without any tenderness. Cardiac and pulmonary auscultation were normal. No neurological abnormalities, adenopathy or rash were detected. Initial blood analysis showed slight inflammation, elevated lactate dehydrogenase level and altered hepatic function (details in the ‘Investigations’ section). Blood gases indicated lactic acidosis and hypoxaemia: pH 7.42, PaCO2 28 mm Hg, PaO2 68 mm Hg, lactate 4.5 mmol/L. Computed tomography (CT) of pulmonary arteries was negative for pulmonary embolism and the pulmonary parenchyma was normal. Research to identify potential infectious causes was conducted. After initial investigations, the patient was admitted to the department of internal medicine without any diagnosis.
Abdominal ultrasound and CT suggested low blood flow in dilated portal and sushepatic veins though they were both permeable. In addition, the walls of the duodenum and gall bladder appeared thickened. Cardiac ultrasound, otherwise normal, showed a delayed contrast passage between the right and left cavities, suggesting an extracardiac shunt, explaining the patient’s platypnoea. With no evidence of infection and no clear diagnosis, examination of bone marrow was carried out and revealed that 25% of the cells were abnormal, large-sized with elevated nucleus/cytoplasm ratios. Unfortunately, no immunohistochemistry could be performed due to technical issues. Peripheral lymphocyte smear did not show any monoclonality.
After 72 hours, though clinically and haemodynamically stable, lactate dehydrogenase levels, lactic acidosis and liver function test results got worse, reaching worrisome values: platelets 42x109/L, albumin 24 g/L, aspartate transaminase 800 IU/L, alkaline phosphatase and γ-glutamyl-transferase of 696 IU/L and 804 IU/L, respectively, lactate dehydrogenase 2008 IU/L, and lactate up to 8 mmol/L. The patient was admitted to the intensive care unit. A transjugular liver biopsy was undertaken to search for a diagnosis. The patient’s hepatic venous pressure gradient (HVPG) was 5 mm Hg. Anatomopathological examination revealed a parenchymal invasion by large CD20+ lymphomatous cells (figure 1). The immunohistological profile was compatible with an IVLBCL, non-germinal center type (ABC-type B-cells by the Hans algorithm): AE1/AE3 (−), CD3 (−), CD20 (+), CD10 (−), BCL6 (+/−), BCL2 (+), MUM1 (+>40%), anti-Ki67 (100%).7 Detection of c-MYC rearrangement by fluorescence in situ hybridisation (FISH using LSI C-MYC Break Apart probes) was negative. Unfortunately, testing for BCL-2 rearrangement could not be performed due to technical reasons. An initial ¹⁸F-fluorodeoxyglucose positron emission tomography – CT (¹⁸F-FDG PET/CT) was performed after the first round of chemotherapy and the only metabolically active signal was a pulmonary-pleural focal point in the right upper lobe (figure 2). Investigations for possible central nervous system infection by brain MR and lumbar puncture were negative.

Transjugular liver biopsy. Immunohistochemistry: CD20 positivity and Hematoxylin and Eosin staining. Nodular and sinusoidal parenchymatous invasion by large lymphomatous cells.
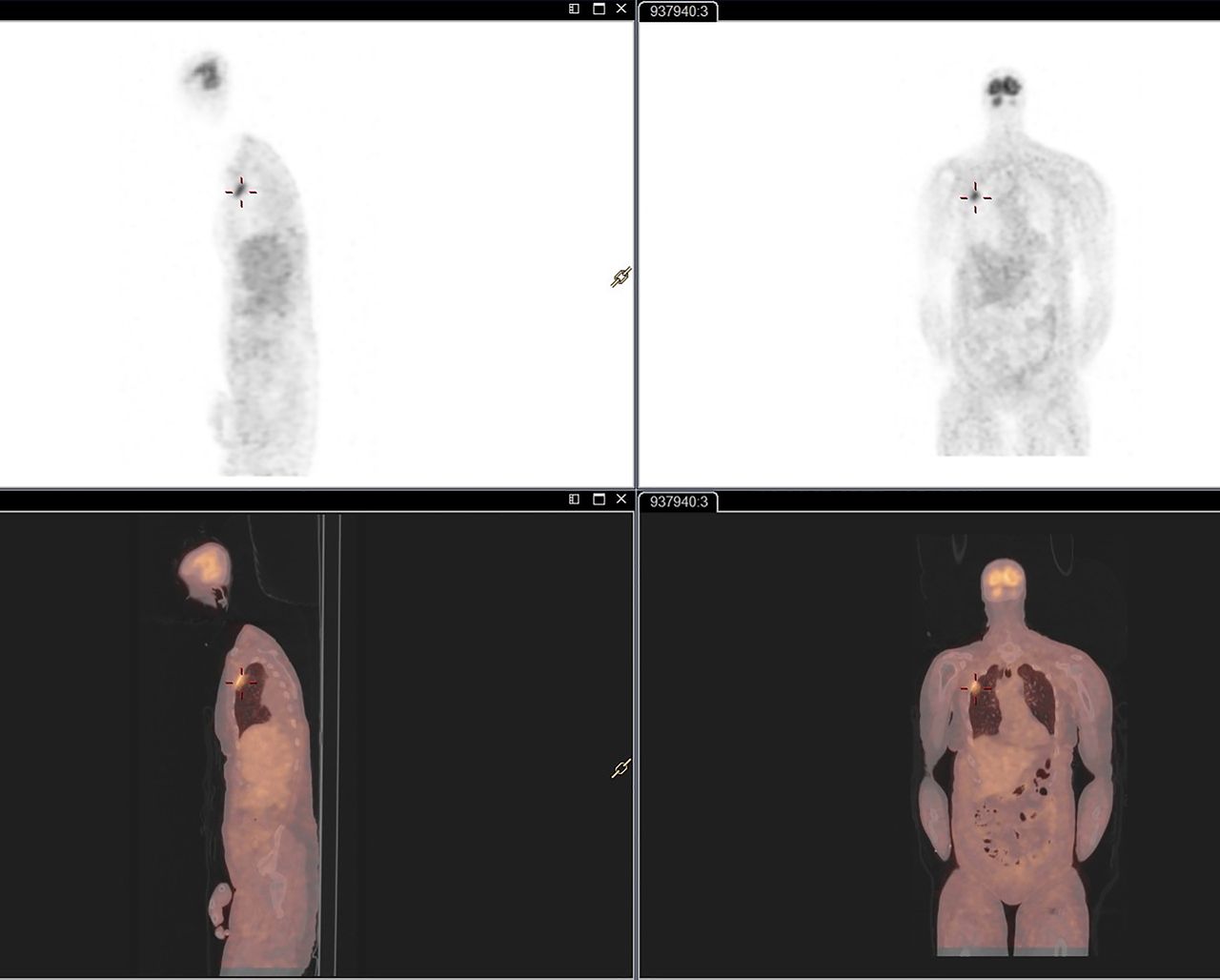
The first fluorodeoxyglucose positron emission tomography—CT was performed after the first round of chemotherapy with the only metabolically active signal a pulmonary-pleural focal point in the right upper lobe.
Investigations
Blood tests at admission: haemoglobin 155 g/L, platelets 168 x109/L, haematocrit 46.2%, WCC 6.3x109/L, neutrophils 4.7x109/L, eosinophils 0x109/L, D-dimers 802 ng/mL, prothrombin time 67%, C reactive protein 88 mg/mL, urea 34 mg/dL, creatinine 0.8 mg/dL, sodium 136 mmol/L, potassium 4.2 mmol/L, chlorine 94 mmol/L, albumin 35 g/L, total bilirubin 0.87 mg/dL, haptoglobin 138 mg/dL, total CO2 19 mmol/L, uric acid 5.2 mg/dL, lipase 31 IU/L, γ-glutamyl-transferase 356 U/L, alkaline phosphatase 289 U/L, aspartate transaminase 112 U/L, alanine transaminase 88 U/L, lactate dehydrogenase 798 U/L.
Differential diagnosis
The patient’s travel history, fever and elevation of serum lactate levels led us to search for sepsis and infectious causes with liver involvement. Urinary, blood cultures and a broad spectrum of analyses were carried out including: Plasmodium spp, hepatitis A virus (HAV), hepatitis B virus (HBV), hepatitis C virus(HCV), hepatitis E virus (HEV), cytomegalovirus (CMV), Epstein-Barr (EBV), human immunodeficiency virus (HIV), typhoid fever, Chikungunya, West Nile virus, Brucellosis, Q-fever, Bartonellosis, dengue fever, Entamoeba histolytica, Leptospira biflexa, Leishmania donovani, Ascaris lumbricoides, Fasciola hepatica, Schistosoma mansoni, Strongyloides stercoralis, Toxocara canis, Chlamydia pneumoniae, Mycoplasma pneumoniae. All of these investigations came back negative. The absence of eosinophilia and no focal lesions in the liver made parasitic aetiologies improbable. The absence of rash, arthralgia, high levels of inflammation, and high-grade fever was not in favour of malaria, viral fever or bacterial causes. Deep infectious foci and endocarditis were excluded by chest and abdominal CT and echocardiography. Sepsis was considered, but with a relatively good general condition, without any clear source of infection and no haemodynamic instability, it was thought improbable.
The second set of diagnoses that were initially considered included pulmonary embolism and/or cardiac involvement with liver impact. These were excluded by chest CT and echocardiography.
Toxic hepatitis and autoimmune disorders were also considered but anamnesis for exposure and blood screening for autoimmune conditions were negative.
Neoplastic aetiologies, though foreseen since admission, became seriously suspected after the different above-mentioned diagnoses were excluded and given the high levels of lactate dehydrogenase. The results of the medullar puncture confirmed malignancy despite the fact that no clear identification of the neoplastic cells could by performed because of technical issues. The worsening of liver function test results motivated us to perform a liver biopsy and enabled us to arrive at the final diagnosis.
Treatment
The patient was treated for an intravascular diffuse large B-cell lymphoma with liver, bone marrow and possibly small bowel and lung involvement, with possible ‘hepatopulmonary-like’ syndrome. She received an urgent course of cyclophosphamide 750 mg/m2, etoposide 100 mg/m2 and methylprednisolone in the intensive care unit, followed by rituximab 375 mg/m2 and doxorubicin 50 mg/m2 in the haematology department.
The patient received eight cycles of rituximab, cyclophosphamide, doxorubicin, vincristine, methylprednisolone (R-CHOP) (rituximab 375 mg/m2, cyclophosphamide 750 mg/m2, doxorubicin 50 mg/m2, vincristin 1–1.4 mg/m2, methylprednisolone 80 mg every day for 5 days) and standard supportive care. Given the high International Prognostic Index, two cycles of high-dose methotrexate were administered for meningeal prophylaxis, with a 2-week interval, 1500 mg/m2.
Outcome and follow-up
Clinical and biological responses were rapidly achieved after the first course of chemotherapy. All biological abnormalities resolved and the patient felt well enough to be discharged 11 days after admission. Clinical and biological follow-up was performed at least once a month and ¹⁸F-FDG PET/CT was carried out twice during the 6 months of therapy. Complete remission was confirmed by ¹⁸F-FDG PET/CT 7 months after initial presentation and after the last of the eight cycles of R-CHOP.
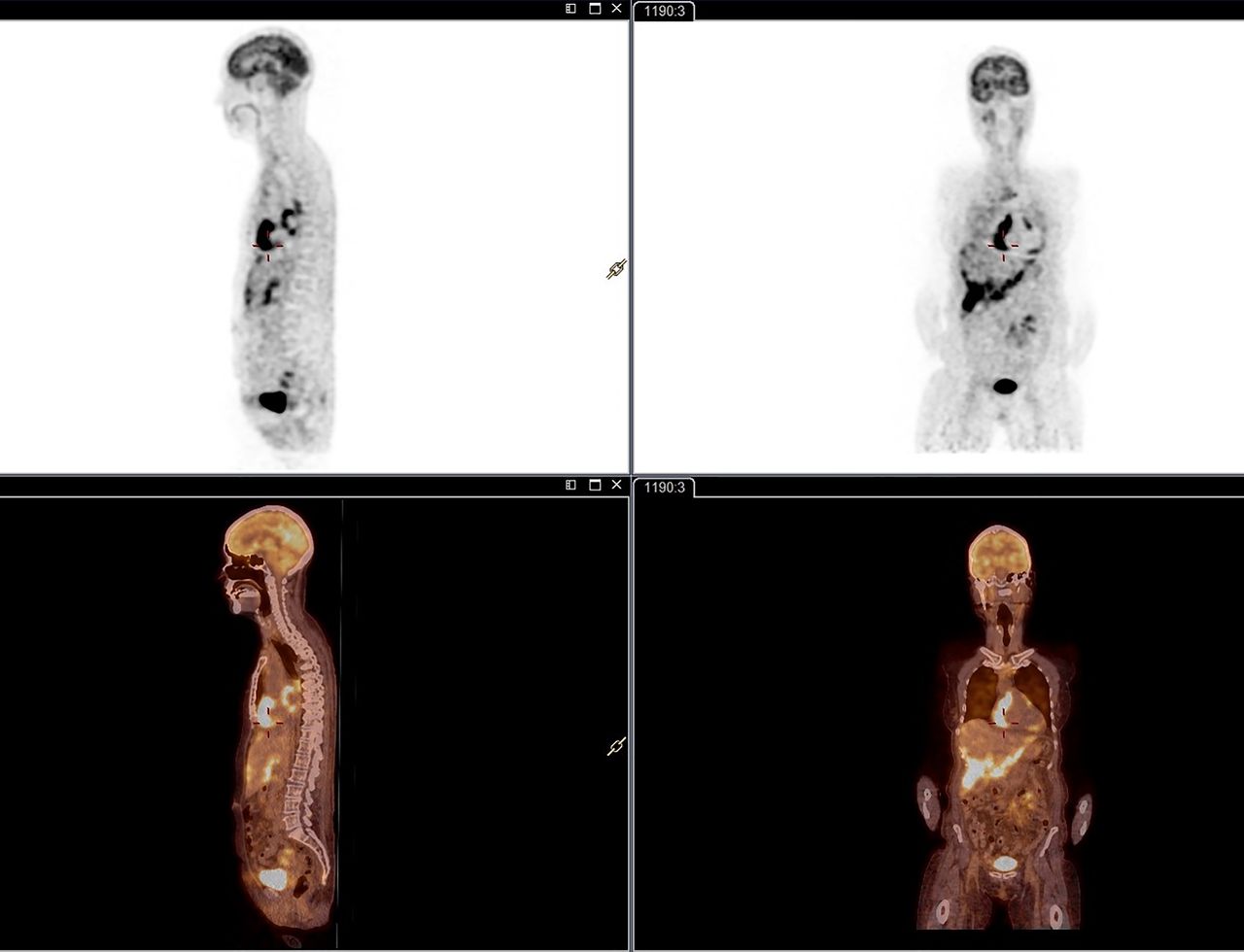
Nine months after treatment and complete remission, the patient presented with general malaise, abdominal discomfort, diarrhoea and dyspnoea with severe hypoxaemia with the following blood gas values: pH 7.45, PaCO2 36 mm Hg, PaO2 43 mmHg, lactate 3.5 mmol/L. ECG showed an atrial flutter, chest CT showed bilateral ground glass opacities (figure 3), ¹⁸F-FDG PET/CT suggested massive lymphomatous relapse: new cervical, mediastinal, abdominal bilateral lymphadenopathies and hypermetabolic spans in the pericardium, lungs, liver, bones, peritoneum and retroperitoneal area (figure 4). Since the images of the chest CT were suspicious, bronchoalveolar lavage was carried out to rule out opportunistic infections. Bone marrow examination was negative but trans-bronchial biopsies confirmed the same neoplastic cells as in the initial liver biopsy. The patient received two rounds of rituximab, revlimid, iphosphamide, carboplatin, etoposide (ICE) chemotherapy and two rounds of rituximab-ICE) for relapse of IVLBCL. Tolerance to treatment was acceptable except for the presence of peripheral sensory polyneuropathy. The patient responded well to therapy and went home a few weeks after admission. After 4 months, complete clinical, biological, and radiological remission was achieved once again. Patient is still in complete remission 2 years after last chemotherapy.

Chest CT at relapse showed pericardial effusion and ground glass bilateral opacities.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
¹⁸F-fluorodeoxyglucose positron emission tomography—CT at relapse: new cervical, mediastinal, abdominal bilateral lymphadenopathies and hypermetabolic spans in pericardium, lungs, liver, bones, peritoneum and retroperitoneal area.
Discussion
This case of IVLBCL that we have described is categorised as ‘classical’ type in the recently proposed classification of three clinical types of IVLBCL: multiple organ involvement without HS.4 In a recent review of 10 cases of ‘non-mainly cutaneous’ IVLBCL the main biological and clinical features were fever, weight loss, night sweats, cytopenia, skin and neurological signs in patients of a median age of 67 years old without significant sex prevalence and a high International Prognosis Index.6 These findings are consistent with most of the other case series, where elevated LDH levels and splenomegaly are common features.5 8 9 Our case presents some interesting features.
First, to our knowledge, only one other case of orthodeoxia associated with IVLBCL has been well-described in the literature.10 In our case, this sign might be associated with an ‘hepatopulmonary-like syndrome’ usually described in advanced liver disease, even if the HVPG of 5 mm Hg observed in our patient is usually considered to be the upper limit of normal.11 12 The low blood flow in a globally dilated venous portal and sushepatic network in the abdominal imaging by ultrasound and CT, without any description of pulmonary hypertension, might also be a clue in favour of such a hypothesis. However, even though this is interesting from a physiological perspective, understanding the details of this theory probably has no clinical implications and these radiological signs were not included in the follow-up.
Second, the patient had biopsy-proven bone marrow, liver, and lung involvement, despite no radiological signs in these organs at initial presentation. As cytopenia of one or more cell lines is a common feature of classical IVLBCL, bone marrow is a frequent site of biopsy and is reported as an affected organ.6 ¹⁸F-FDG-PET seems to be critical, but not perfect, for evaluation of the extent of IVLBCL.13 However, standard radiological findings that enable targeted biopsy of liver and lung do not always provide good correlations with involvement of these organs; random biopsies (or autopsies) can sometimes be positive.14–16 Moreover, our patient did not present any abnormalities in the different cell lines and thrombocytopenia was related to hepatic dysfunction. This is also consistent with the positivity of random skin biopsies in some case series.17 This might reflect a wider extent of the disease than that suggested by radiological findings, perhaps related to the physiopathology of IVLBCL which involves cells located in small and intermediate blood vessels.2 Any unexplained sign, whether radiological, biological or clinical, might motivate clinicians to perform a biopsy that could be positive. This discussion is complicated in our case by the timing of the first ¹⁸F-FDG PET/CT, which might have been positive if performed before the first course of chemotherapy. Finally, pericardial involvement, at the forefront during the relapse of the disease in this case, seems to be uncommon, or underreported in published series.5 9 17
Another unique feature of this presentation was lactic acidosis. While usually due to tissue hypoxia or sepsis and referred as ‘type A’ lactic acidosis, ‘type B’ lactic acidosis can be infrequently related to malignancy, as in our case.18 The majority of lactic acidosis related to haematological neoplasms is usually associated with poor prognosis.19 Obviously, it can be difficult to differentiate the cause of elevated blood lactate in critically ill patients suffering from cancer, since they might concomitantly be affected by malignancy and sepsis. Our patient showed no sign of infection whatsoever and few clear descriptions of similar reports are available in literature.19 20 However, altered hepatic lactate clearance related to liver dysfunction might have played an important role in this case.
In conclusion, this case of IVLBCL highlights important features that should raise suspicion of this malignancy during the differential diagnosis. In particular, the presence of platypnoea, the presence of lactic acidosis in the absence of infection, and the presence of clinical or biological signs that are not explained by radiological findings should lead to additional follow-up. IVLBCL may respond well to treatment, if detected in a timely manner.
Patient’s perspective
‘I had this impression that I had never been really sick. I have always thought that I was in excellent health and could get through anything…
At first, as I was taking a walk, I felt that I was short of breath at the slightest little hill. Two days later, we went abroad. On our arrival, our family welcomes us with a delicious meal but in the evening already, when I was about to go to bed, I felt heavy. The following day, I was feeling a little nauseous, I took a nap, which I rarely do, and I threw up for the first time. Then, little by little, I had difficulty going up the stairs, I had to sit down after a few steps, I was out of breath. Finally, the day after, we went to the emergency of a local hospital. They took me in charge right away and after some exams, they told me that either they were keeping me there and had me transferred to a bigger city, or I needed to return immediately and go to a hospital back home. This is what we did. My husband and a friend were driving alternately for the trip (during which I was throwing up at each stop …) and dropped me off at a university hospital at 4:00 in the morning. I had trouble breathing and also felt pain under my ribs. But there, at the hospital, I felt reassured. For a few days, my condition was getting really worse, I felt I was slowly leaving, but I had total trust. The doctors could not understand what I was suffering of, they were still searching. Easter weekend was coming closer and people were leaving for holidays. They asked a specialist to come back in order to perform to me a liver puncture. Same thing for the analysis, it could not wait until the end of the weekend. Finally, on Sunday evening the chemotherapy started, just in time and there I felt that everything was going up again. And I was coping well with them. I stayed in the hospital for another fortnight. As I was very weak and had not eaten for 10 days, it took me some time to recover, when I got home, but everything ended well, 7 months later.
The following summer, I started having new disturbance, tiredness, shortness of breath; I was getting weaker, but less quickly than the first time. We were once again on holidays and we definitely did not expect that the lymphoma was going to attack me again.
After a telephone consultation with my oncologist, we returned home and went once again to the hospital. There, I had a lot of exams, some of them quite hurtful, in order to eliminate different scenarios but in the end, we realised that the lymphoma was there again and the treatment started again. I think that I have being taken in charge in a marvellous way, both by my oncologist and by the various doctors and the team of nurses.
But I still do not understand why these lymphomas attacked me, since I have always eaten in a balanced way without too much fat, without too much meat, with a lot of vegetables, I am active, I am not overweight, … well, everything that is recommended.’
Learning points
Intravascular large B-cell lymphoma (IVLBCL) is a rare but life-threatening condition and prompt diagnosis is necessary for rapid treatment.
Clinical presentation is extranodal and variable in space and time. Diagnosis is challenging, IVLBCL should be kept in mind early in differential diagnosis of syndromes with unclear aetiologies.
Imaging, though necessary to progress towards definite diagnosis, is not perfectly sensitive and investigations should be made according to clinical and/or biological signs.
The extent of the disease is possibly wider than expected based on radiology. Random biopsies, in particular of the lungs and skin, should be performed according to unexplained biological or clinical features.
Despite a quick response, close follow-up should be set up as good responses to treatment do not guarantee absence of early relapse.
Ethics statements
References
Footnotes
Contributors The first author was involved in the initial clinical management and responsible for the drafting process and literature review. The third author was responsible of reviewing the last version of the article. Both other authors were in charge of the diagnosis, clinical management and treatment of the patient.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.