Article Text

Statistics from Altmetric.com
- pulmonary emphysema
- interstitial lung disease
- rheumatoid arthritis
- connective tissue disease
- rheumatology
Description
A 66-year-old man with rheumatoid arthritis (RA) and chronic obstructive pulmonary disease (COPD) presented to our hospital with exertional dyspnoea. He smoked three packs a day for 34 years until he was diagnosed with RA and COPD at the age of 54. He still smokes a half pack a day. RA was in remission but had been in high activity until the administration of abatacept at the age of 63. COPD was treated by a long-acting β2 agonist and long-acting muscarinic antagonists; however, the modified Medical Research Council dyspnoea scale was grade 3. On physical examination, we found that he breathed by the shoulder, using accessory muscles. His respiratory sound was lowered in the bilateral upper lungs. However, fine crackles were heard in late inspiration in the bilateral lower lungs. He had club fingers without tenderness and swelling in the joints. Arterial blood gas analysis in room air revealed that arterial oxygen tension and alveolar carbon dioxide tension were 56.0 mm Hg and 33.1 mm Hg, respectively. Chest X-ray radiography revealed bilateral reticular opacities in the lower lungs (figure 1). CT revealed severe emphysema in bilateral upper lobes and interstitial fibrotic changes in bilateral lower lobes (figure 2). However, there was no evidence of lung cancer. The respiratory function test revealed forced expiratory volume in 1 s (FEV1) of 78.3%, forced vital capacity (FVC) of 87.5% and FEV1/FVC ratio of 72.5%. The diffusing capacity of the lung for carbon monoxide (DLCO) was 37.8%. He was diagnosed with combined pulmonary fibrosis and emphysema (CPFE). Ultrasonic echocardiography revealed that estimated right ventricular systolic pressure was within the normal range (33.8 mm Hg). Home oxygen therapy was initiated in addition to counselling on smoking cessation.

Bilateral reticular opacities in the lower lungs on chest X-ray radiography.
{kind=link}
{kind=link}
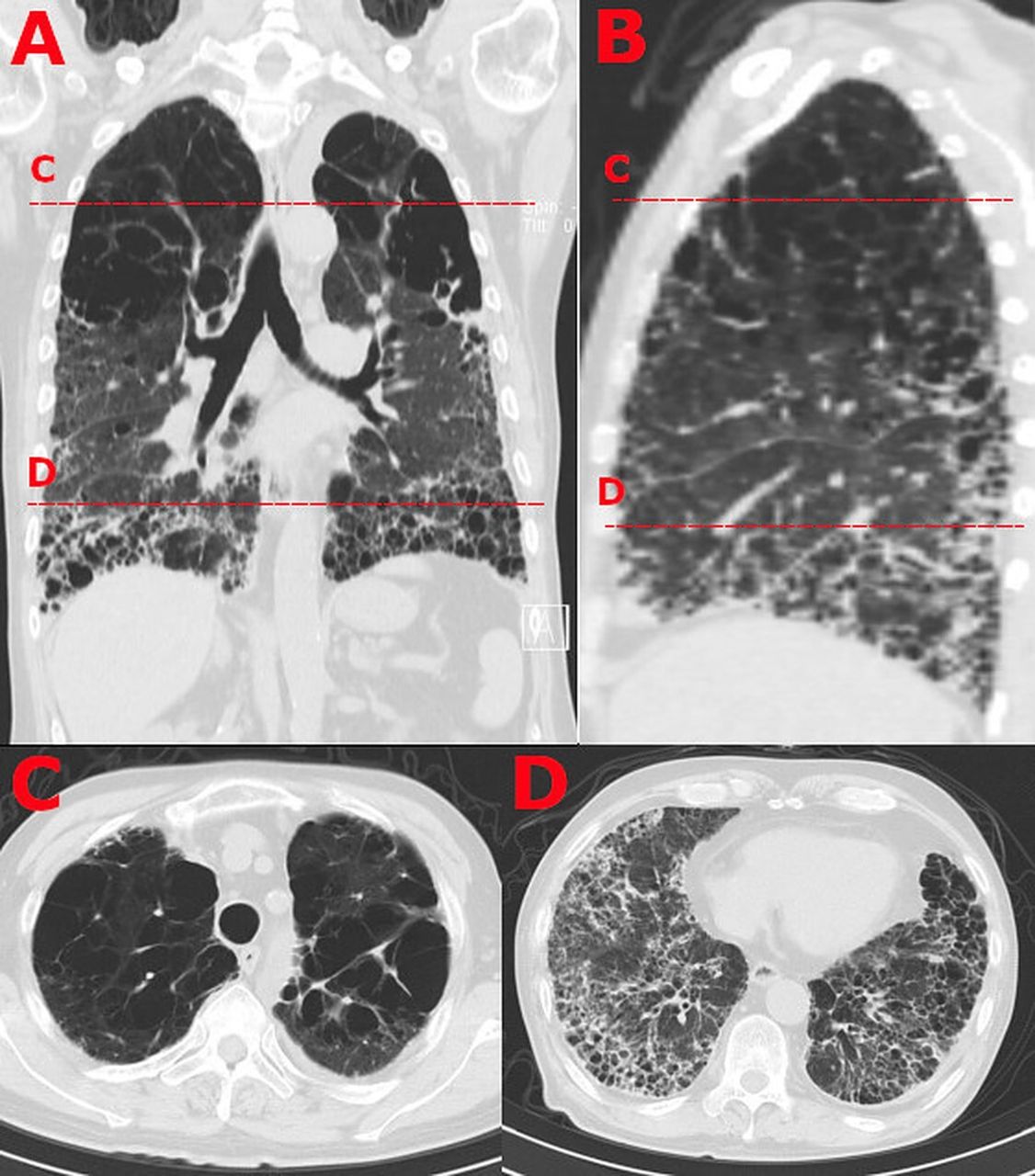
Centrilobular and paraseptal emphysema in the bilateral upper lobes and reticular opacities and honeycombing in the bilateral lower lobes on CT. (A) Bilateral lungs on coronal plane with axial level of section (C, D). (B) Right lungs on sagittal plane with axial level of section (C, D). (C) Bilateral upper lobes on axial plane. (D) Bilateral lower lobes on axial plane.
CPFE is characterised by a combination of emphysema of the upper lobes and fibrosis of the lower lobes. Patients with CPFE are mostly men with a current or past smoking habit. Emphysema increases lung compliance, whereas pulmonary fibrosis decreases lung compliance. Therefore, FVC and FEV1 are counterbalanced in CPFE although chest CT shows evident emphysema and fibrosis. DLCO is decreased, reflecting the reduced function of the alveolar-capillary units and alveolar membrane thickening. RA accounts for 53% of the patients with connective tissue disease (CTD) who also have CPFE.1 Compared with idiopathic CPFE, patients with CTD-related CPFE are likely to be younger women with a more favourable prognosis. This may result from earlier recognition of lung disease related to connective tissue disease.1 2 However, CPFE may be associated with a high risk of mortality in RA because DLCO is more decreased in RA-related CPFE than that of RA-related interstitial lung diseases due to the additional emphysematous change.
This case clearly illustrates the dissociation between radiographic change and preserved lung volume in spirometry. We should, therefore, pay attention to DLCO and the association between RA and CPFE.
Learning points
Forced vital capacity and forced expiratory volume in 1 s are counterbalanced in combined pulmonary fibrosis and emphysema (CPFE).
Diffusing capacity of the lung for carbon monoxide is more decreased in rheumatoid arthritis (RA)-related CPFE compared with RA-related interstitial lung diseases.
Ethics statements
Patient consent for publication
Footnotes
Contributors NY and AD made substantial contributions to conception and design and have been involved in drafting the manuscript. KH approved the final version to be published.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Disclaimer Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.