Article Text

Statistics from Altmetric.com
Description
A previously well 21-year-old woman presents with 2 months of a non-tender lump in the left lower neck. On examination, a soft nodule was palpated at the left thyroid gland region. The patient was clinically and biochemically euthyroid. Further evaluation with thyroid ultrasound revealed a solitary large solid-cystic nodule occupying the left lobe-isthmus (figure 1). No cervical lymphadenopathy was evident. Fine-needle aspiration cytology (FNAC) of this nodule yielded haemorrhagic contents. The nodule was followed up on ultrasound over the next 3 years, which demonstrated progressive shrinkage of the nodule’s cystic portions and replacement with iso-to-hypoechoic contents and calcifications. The nodule was deemed suspicious for malignancy and classified as a TR-5 nodule according to the thyroid imaging reporting and data system (ACR-TIRADS) (figure 1C). Repeat FNAC targeting the solid portions was performed, yielding non-diagnostic acellular contents. At latest follow-up, the nodule continued to be smaller and showed degenerative changes, overall compatible with benign mummification.

Baseline thyroid ultrasound in October 2017 (A) showed a solitary mixed solid-cystic nodule (denoted n1 on hand drawn diagram) with mild peripheral vascularity, mainly occupying the left lobe with extension into the isthmus. There is no extrathyroidal invasion. The thyroid gland showed normal appearance. Subsequent sonographic follow-up showed progressive nodule shrinkage and was thereafter confined to the isthmus (B). However, during follow-up in April 2019, the nodule demonstrated ‘suspicious’ features: gently lobulated margins (two points), almost solid composition (two points), hypoechoic echotexture (two points) and punctate echogenic foci suggestive of microcalcifications (three points), hence classified as a TR-5 nodule (total of nine points) (C). Repeat FNAC of the nodule targeting its internal echogenic components was performed (D). Latest follow-up in December 2020 (E) showed further shrinkage of the nodule with development of a hypoechoic halo due to cystic wall collapse (arrow heads) and eggshell calcifications (arrows) consistent with degenerative changes seen in a mummified nodule. FNAC, fine-needle aspiration cytology.
Benign thyroid nodules (eg, hypoplastic/colloid nodule or follicular adenoma) may undergo mummification or degeneration over time, either spontaneously, where cystic portions become desiccated (figure 2), or following FNAC, percutaneous ethanol or laser ablation of solid portions. In mummified solid components, their vascular supply is disrupted, resulting in intranodular hypoxia, haemorrhage and subsequent scarring.1 Various sonographic features of mummified thyroid nodules have been reported, but typically include necrosis associated shrinkage and avascularity, posterior shadowing, as well as regular peripheral black and white halos corresponding to subcapsular granulation tissue and dystrophic eggshell calcifications, respectively.1–4 As benign nodules mummify, some of their morphological changes can resemble or mimic malignancy. For example, mummified nodules may demonstrate irregular ill-defined nodule margins due to capsular collapse, taller-than-wide shape from asymmetric fibrous healing with transverse shrinking, replacement of cystic contents with iso-to-hypoechoic ‘solid’ contents due to fibrosis and internal echogenic foci attributed to dystrophic calcifications or colloid material, usually seen in later stages. Nodule shrinkage, a key feature of mummification, may rarely be seen in papillary thyroid carcinomas.1 4 These features overlap with and may be mistaken for malignancy, or be assigned a falsely high TR score. In turn, this may lead to unnecessary invasive interventions such as repeat FNAC or surgery.
{kind=link}
{kind=link}
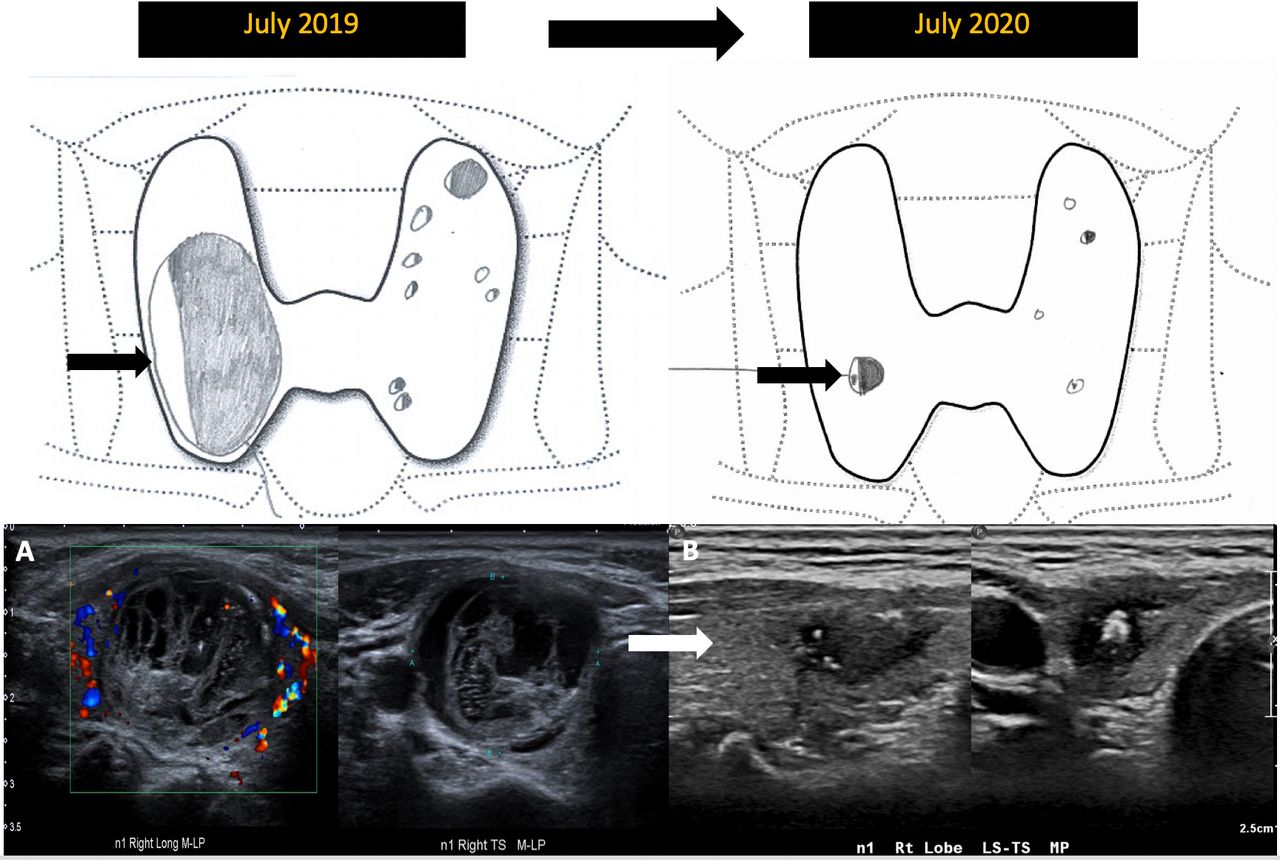
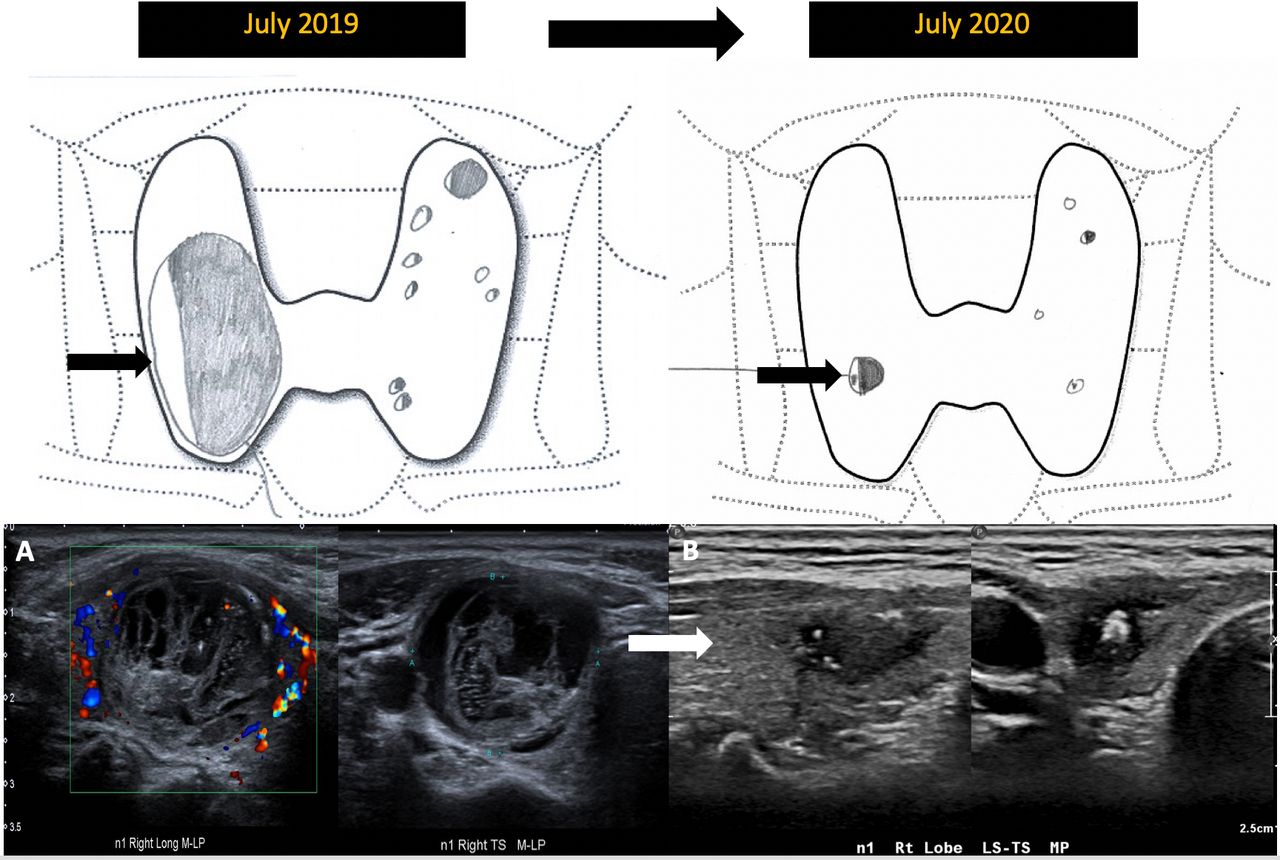
Example of spontaneous mummification of a benign nodule in another 60-year-old female patient with known multinodular goitre. The dominant nodule noted in the mid to lower pole of the right thyroid lobe initially appeared predominantly isoechoic, almost entirely solid, wider-than-tall with smooth margins. Minor internal vascularity and several large comet tail artefacts were also seen, overall in keeping with a colloid nodule (A) At 1-year follow-up, the nodule shrank significantly, appeared hypoechoic and developed increased internal echogenic foci with comet tail artefacts, consistent with degeneration or mummification (B).
Hence, distinguishing mummification from malignancy is important. Some features which are highly specific for mummified nodules include the ‘cystic wall shrinkage’ sign, referring to the slightly wavy, often incomplete hyperechoic halo at the nodule edge; the ‘inner isoechoic rim’ sign, a thin continuous isoechoic rim along the inner margin of the intact solid wall of pre-existing cystic nodules; and the ‘halo’ sign, denoting the hypoechoic rim around the outer margin of the nodule due to a compressed fibrotic pseudocapsule, etc.3 4 Other clues, including the absence of any associated suspicious lymphadenopathy or intralesional vascularity, especially when combined with FNAC results that are repeatedly non-diagnostic or insufficient, will also help clinch the diagnosis, as demonstrated in our case.
Thus, this case highlights the importance of meticulously reviewing prior comparison imaging, especially for nodules exhibiting shrinkage and morphological changes following intervention, so as to correctly identify the process of mummification and prevent any unneeded invasive management. For nodules that remain suspicious, histological evaluation with tissue sampling should be considered.
Learning points
Benign thyroid nodules can mummify either spontaneously, following fine-needle aspiration cytology (FNAC) or percutaneous ethanol injection/ablation. The morphological changes of mummification can mimic malignancy and result in unnecessary invasive interventions.
Certain ultrasound features may suggest mummification. The absence of intranodular vascularisation and suspicious regional lymph nodes, along with progressive nodule shrinkage and benign/non-diagnostic FNAC results however favours mummification over malignancy.
Follow-up ultrasound imaging should be performed first for nodules demonstrating shrinkage and changes in echotexture on prior comparison studies. Tissue sampling for histological diagnosis should be reserved for nodules that remain suspicious (eg, with increasing solid component or internal vascularity).
Ethics statements
Patient consent for publication
Footnotes
Contributors TSET conceptualised and drafted the manuscript. SKS critically reviewed and revised the manuscript. All authors contributed to finalising the manuscript as submitted.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.