Article Text

Abstract
Erysipelothrix rhusiopathiae transmission to human is often occupation-related, but in most cases, a detailed case history is missing. This case report is based on an interdisciplinary approach and includes a thorough medical record. A 58-year-old laboratory technician working on geese necropsy cut open her glove at a rib fragment of a goose and subsequently noticed a slowly progressive, reddish skin alteration in the particular region of the hand. Bacteriological investigations on the geese revealed septicaemia due to E. rhusiopathiae and therefore substantiated the diagnosis of the patient. The infectious agent could not be cultured from the patient; however, antibiotic susceptibility testing was performed using the goose isolate. An entire follow-up until full recovery of the patient was conducted. Zoonotic infections possibly have a significant impact on certain occupations. This case report analyses a rare but important zoonotic infection to create awareness of this in physicians caring for human patients.
- occupational and environmental medicine
- infectious diseases
- accidents
- injuries
- dermatological
- disease and health outcomes
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- occupational and environmental medicine
- infectious diseases
- accidents
- injuries
- dermatological
- disease and health outcomes
Background
Erysipelothrix rhusiopathiae transmission to human has been known for more than a century1 and is often occupation-related by direct contact with faeces, saliva or nasal discharge of infected animals. Nevertheless, recognition and diagnosis of this possible life-threatening bacterial zoonosis is still challenging, especially if a clear case history is missing. The herein presented case report of a laboratory technician being infected while performing geese necropsy is based on an interdisciplinary approach and displays a detailed medical history. The authors aim to maintain awareness of this infrequent but potentially severe disease and highlight the beneficial effects of cooperation between veterinarians and physicians.
Case presentation
A 58-year-old woman without pre-existing medical condition presented to the emergency department (ED) of a tertiary hospital with a reddish skin alteration at the right interdigital space. Eleven days earlier, she was working as a laboratory technician in the necropsy hall of a faculty of veterinary medicine where she sustained a minor skin wound while working on geese necropsy. That day, four 6-month-old geese were submitted for diagnostic pathological examination. The flock consisted of 350 geese whereof four animals died within 12 hours without any previous clinical signs. Submissions due to mass mortality events among birds are suspicious for highly contagious and potentially zoonotic diseases, such as avian influenza (AI, influenza A virus) or Newcastle disease (NCD, avian orthoavulavirus-1). To prevent personnel from zoonotic infections with either AI or NCD, a pen-side Anigen Rapid AIV Ag/NDV Ag Test Kit (BioNote, Hwaseong, South Korea) was performed on cloacal swabs before necropsy started. The tests gave negative results for the above-mentioned infectious diseases that would have required notification to veterinary authorities in Switzerland. Subsequently, two randomly selected carcasses were necropsied. The technician prepared the animals according to routine methods: wet the animals to reduce the risk of inhaling dander potentially bearing pathogens; open the carcasses using a pincette, a scissor and a poultry shear; extract most of the inner organs and open the intestine to perform parasitology. While opening the thorax of one goose, a sharp rib fragment punctured the right protective glove of the patient between digit II and III. Immediate washing and disinfecting of her hands was conducted according to standard procedures.
Investigations
Veterinary examination of the geese carcasses revealed dehydration, moderate to severe chronic ulcerative bilateral pododermatitis, and in one goose, multiple disseminated pericardial haemorrhages. Livers and spleens were congested and the kidneys showed a prominent reticular pattern. Other internal organs, including endocardium, were without specific findings. Parasitological examination of the intestine and the plumage was negative. Culture of heart, liver and lung on sheep blood agar and bacterial identification using matrix-assisted laser desorption/ionisation time-of-flight mass spectrometry (MALDI-TOF-MS) revealed E. rhusiopathiae. The MALDI-TOF-MS scores ranged from 2.02 to 2.15 (excellent match). Thus, erysipelas (a term specifically used in veterinary medicine for skin or disseminated E. rhusiopathiae infections) was established as a cause of death in these geese. Regarding the zoonotic potential, involved personnel were advised to be vigilant about skin changes.
From day 1 after the incident, the patient noticed a slowly progressive, reddish skin alteration where the bone had pierced the glove. On day 11 she reported to the supervisor and was sent to the ED of a tertiary hospital with an accompanying letter describing the circumstances and isolated pathogen.
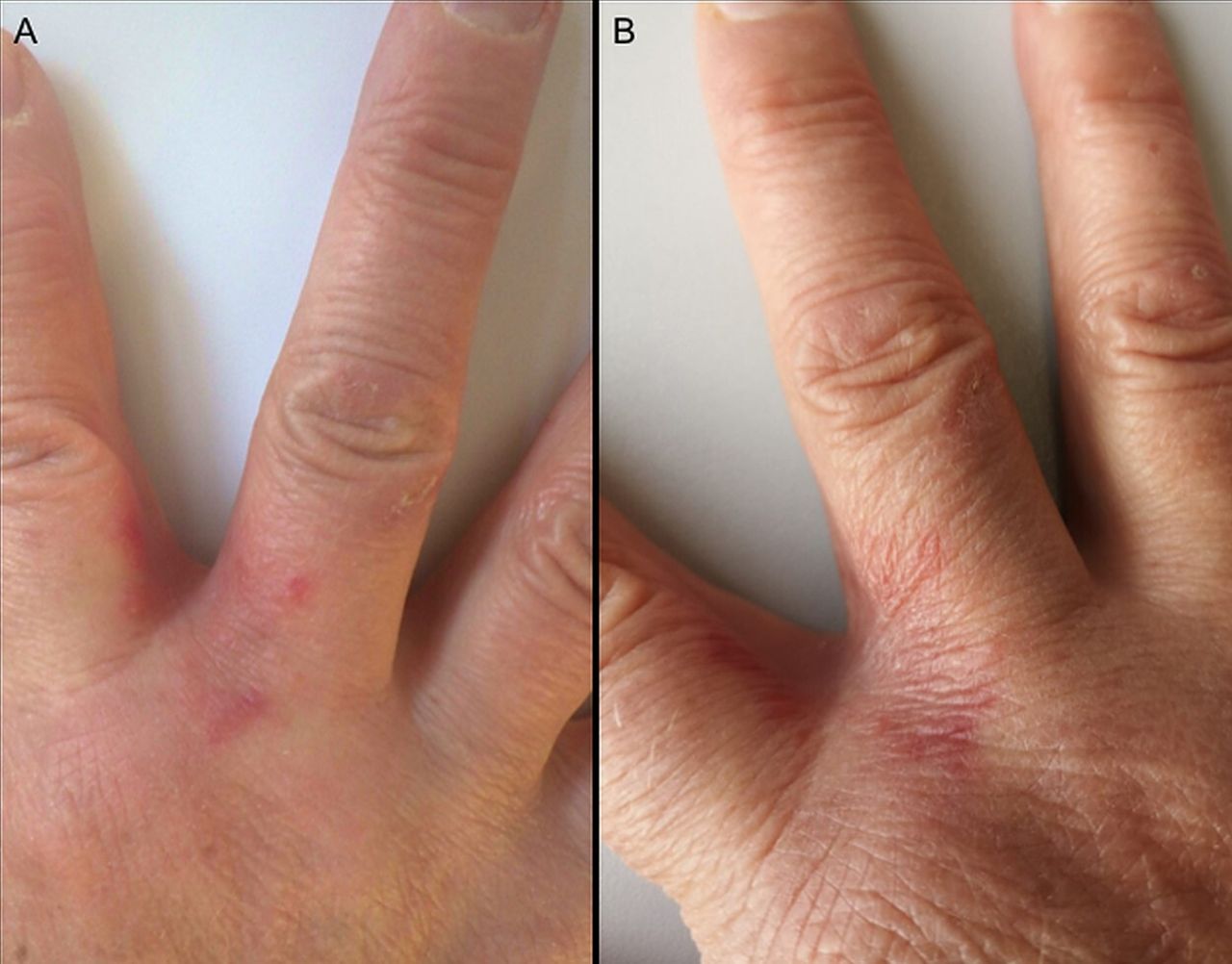
At presentation at the ED, her general condition was good, she reported no fever or night sweats. Clinical examination showed no cardiovascular, pulmonal, gastrointestinal, urogenital or musculoskeletal disorders apart from the skin lesion: between the right digits II and III a strictly delimited erythematous maculopapular discoloration was identified (figure 1A). Digits were neither swollen nor painful, but a mild pruritus was noted. Further routine laboratory tests (haematology, clinical chemistry) were unremarkable and blood cultures remained sterile. Local erysipeloid was diagnosed based on the case history.

{kind=link}
Clinical presentation of Erysipelothrix rhusiopathiae infection. (A) Acute local cellulitis with vesicles between right digits II and III as presented to the hospital on day 11 postinjury; (B) lesions almost resolved on day 15 postinjury.
Differential diagnosis
Transmission of E. rhusiopathiae to human is often occupation-related2–7 (eg, butchers, fishermen, veterinarians, meat-processing workers or pig, sheep and poultry farmers) by direct contact with infected animals.4 8 Therefore, exposure to septic geese in necropsy poses a risk of infection. In humans, three clinical forms of the disease6 9 10 are known. Erysipeloid is the most frequent and induces a mild cutaneous infection with acute localised cellulitis,11 occasionally with vesicles but without suppuration. Less common is the generalised, diffuse cutaneous form with spreading beyond the entry site and bullae formation, often associated with systemic symptoms like fever, joint or muscle pain.12 Rarely, septicaemia with endocarditis occurs in 34% of the severe cases.6 13 On the basis of the patient’s physical examination, erysipeloid was the most probable medical outcome. The pathological and bacteriological examination of the geese strongly substantiated this diagnosis. As a differential diagnosis, erysipelas10 due to infection with streptococci, staphylococci or other bacteria, acute allergic contact dermatitis,10 and scabies, must be considered.
Treatment
The first-line choice antibiotic against local E. rhusiopathiae infections is penicillin or cephalosporin, and clindamycin or fluroquinolones in case of intolerance of penicillin.6 10 14 15 E. rhusiopathiae is resistant to vancomycin, teicoplanin and daptomycin. While blood cultures from the patient remained sterile, an isolate of the goose was analysed for antibiotic susceptibility and showed it to be sensitive to all antibiotics tested (penicillin, ampicillin, ceftiofur, erythromycin, enrofloxacin). Correspondingly, the treatment with amoxicillin three times a day for 1 week was successful. The erysipeloids subsided within 5 days after initiation of treatment (figure 1B).
Outcome and follow-up
In this report, a skin infection with E. rhusiopathiae with known time point of infection and entire follow-up until remission is presented. After full recovery, the patient reported no relapse or late sequelae within 6 months. The bacteriological diagnosis might be challenging, as secondary pathogens may overgrow the small and slow growing colonies of E. rhusiopathiae on agar plates.16 Therefore, the final diagnosis of erysipeloid should be based on the patient’s occupation, previous traumatic contact with infected animals or contaminated objects, characteristic skin lesions with lack of severe systemic illness, laboratory results and rapid healing following treatment.10
Discussion
E. rhusiopathiae is a rod-shaped, Gram-positive, facultative anaerobic, non-motile and non-spore-forming bacterium.12 Various wild and domestic animals, including fish and birds may shed E. rhusiopathiae,2–5 9 but swine are the most important reservoir.8 30%–50% of apparently healthy pigs8 harbour it in the lymphoid tissues of the alimentary tract.8 17 Studies showed that E. rhusiopathiae persists for up to 35 days in soil,12 18 remain viable for 12 days when exposed to direct sunlight and for several months in buried or unburied carcasses.7 8 Infection due to environmental contamination is believed to pose the main threat for transmission.19 E. rhusiopathiae enters the body mainly through acute traumatic or pre-existing skin lesions.12 In our case, the patient had coarse skin where the bone fragment punctured the glove. Similarly, the footpad lesions are supposed to be the most likely entry point in the geese suffering from moderate to severe chronic ulcerative bilateral pododermatitis. Case reports of E. rhusiopathiae outbreaks among geese are scarce.20 21 Similar to our case, they assumed that transmission occurred due to contaminated pasture or soil; either if sheep or swine had priorly been kept in the same barn or on the same pasture, or from excretions of infected wild animals, such as wild fowl, rodents or insects.12 The fast diagnostics allowed rapid intervention on the geese farm, in particular, rotation to another pasture and exchange of the pond water. These measures turned out as effective and no more geese were affected. Interdisciplinary approaches lead also to successful treatment of the laboratory infection, potentially preventing a disseminated infection, such as endocarditis.22 Although erysipeloid skin lesions may resolve spontaneously, antibiotic treatment shortens the duration of local symptoms and may prevent relapse.7 Recommendations regarding prophylaxis after exposure to E. rhusiopathiae are lacking. But exposed individuals should be monitored and, as outlined by the last consensus statement of the Infectious Diseases Society of America,22 antibiotic therapy should immediately be initiated if skin lesions or systemic symptoms occur. Cooperation between veterinarians and physicians are therefore highly recommended to gain greater influence in the future investigation of similar cases.
Learning points
Disease awareness of this infrequent but potentially life-threatening infection with Erysipelothrix rhusiopathiae.
Benefit of cross-disciplinary exchange of results and knowledge.
Awareness of occupation-related diseases and spectrum of occupations potentially affected.
Acknowledgments
The authors would like to thank Daniel A Bossard, MD from the University Hospital Zurich for the valuable assistance in writing the case report and Dr. med. vet. FVH Marianne Schneeberger from the Division of Veterinary Bacteriology at the Vetsuisse Faculty University of Zurich for performing the antibiotic resistance analysis. Furthermore, many thanks to Professor Roger Stephan from the Institute for Food Hygiene and Safety at the Vetsuisse Faculty University of Zurich for the appreciated support.
References
Footnotes
Contributors SMM and SA performed the veterinary examination of the geese. JK and DIK performed the clinical examination of the patient. All authors contributed to the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Disclaimer Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.