Article Text

Statistics from Altmetric.com
Description
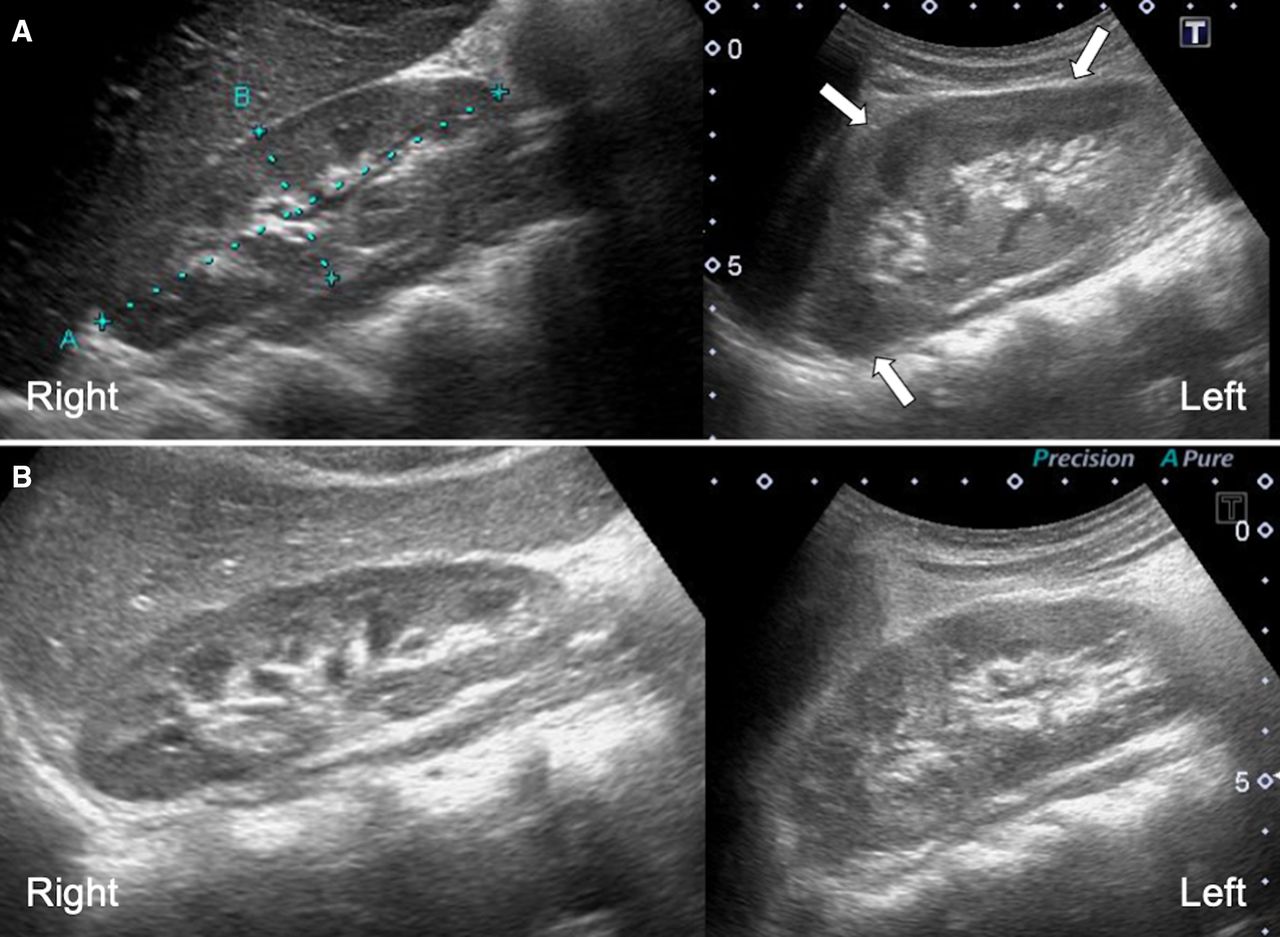
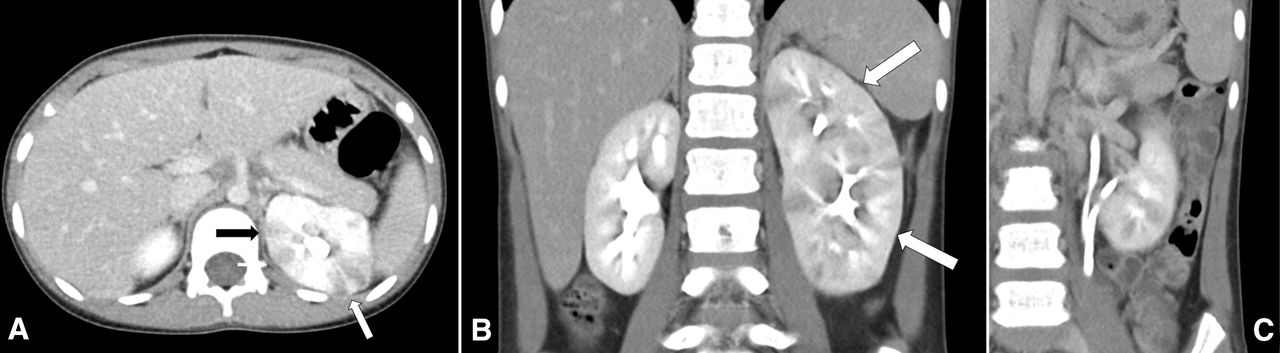
A healthy 8-year-old girl presented to our hospital with fever and vomiting for 5 days. She had no complaint of flank pain during this time. On examination, she appeared exhausted, and the capillary refilling time was prolonged. Laboratory data revealed elevated inflammatory markers (white blood cell (WBC) count, 15.8x109/L; C-reactive protein, 6.5 mg/dL) and pyuria (WBC count >100/high-power field). Gram-negative rods were also identified in urine. Renal ultrasound showed an enlarged left kidney with a hypoechoic lesion, which was suspected to be acute focal bacterial nephritis (AFBN) (figure 1A). Contrast-enhanced CT showed low-density areas in the upper pole of the left kidney, which confirmed the AFBN diagnosis (figure 2A). Hydronephrosis was not observed; however, partial duplication of the ureter and renal pelvis in the left kidney was present (figure 2B,C). Intravenous cefotaxime was initially started but was switched to cefazolin because urine culture detected Escherichia coli sensitive to this antibiotic. Blood culture was negative. The antibiotic course was continued for 3 weeks. Voiding cystourethrogram was not performed, as this was the first episode of urinary tract infection and hydronephrosis was not detected on imaging. She did not have recurrence of urinary tract infection or other complications during the 6-month follow-up period. Renal ultrasound on the 6-month follow-up showed improvement in the hypoechoic lesion; however, the left kidney remained enlarged (figure 1B). We are planning to perform Technetium-99m dimercaptosuccinic acid renal scanning for detecting renal scarring in the future.
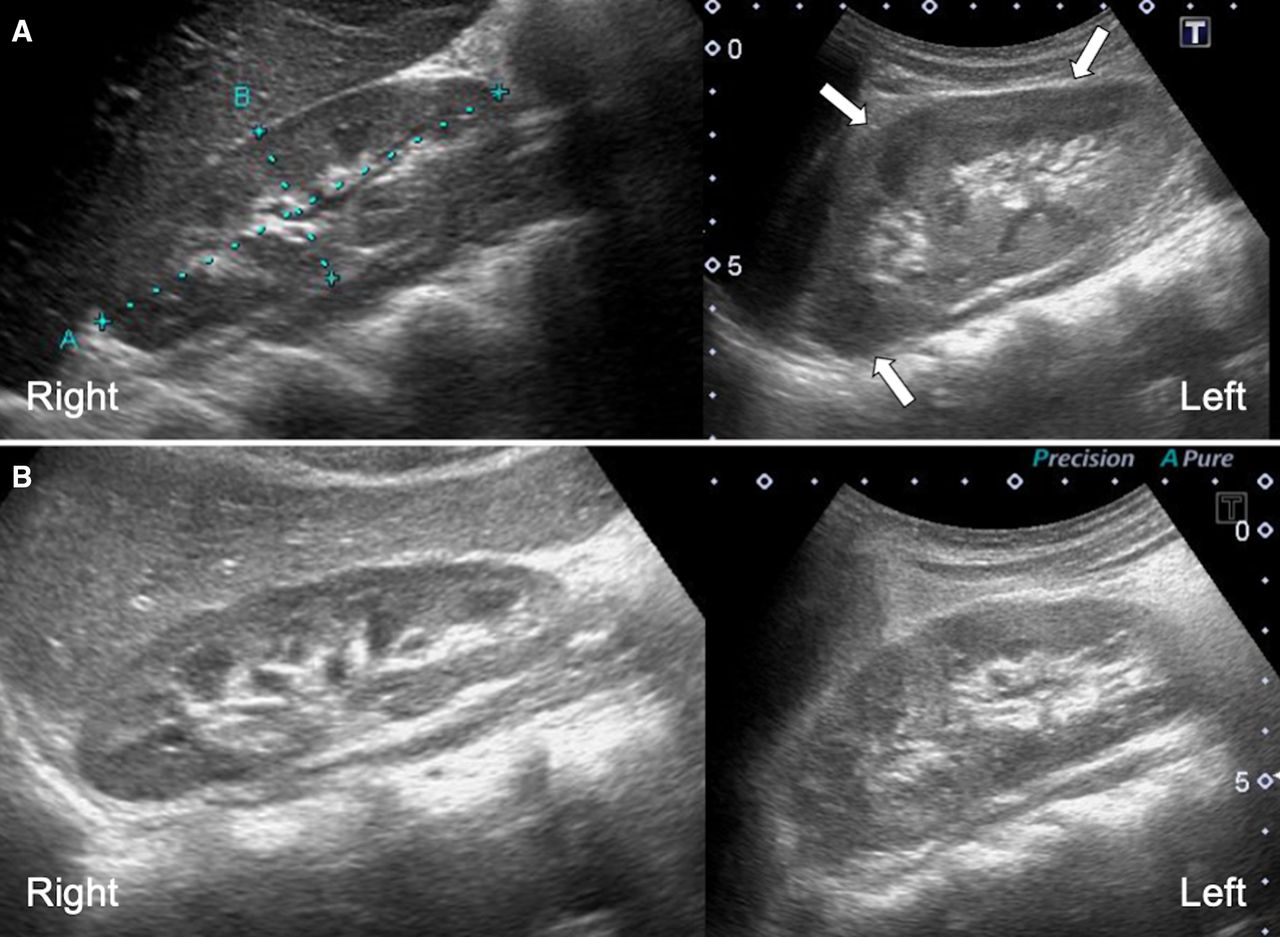
Ultrasonographic findings; (A) initial ultrasound of the patient; an enlarged left kidney (97.8×35.7 mm) with a hypoechoic lesion, which was suspected to be acute focal bacterial nephritis, was detected (arrows). The right kidney had a normal size (79.2×28.4 mm) without any significant abnormality. (B) Ultrasound of the patient on 6-month follow-up; hypoechoic lesions in the left kidney had improved, however, the left kidney remained enlarged (92.7×37.4 mm). The right kidney did not have any abnormality (78.4×26.9 mm).

{kind=link}
{kind=link}
CT scan of the patient; (A) low-density areas were present in the upper poles of the left kidney. (B, C) The left kidney had two separate pelvicalyceal systems and two ureters, which joined before connecting to the bladder. The left kidney was enlarged and appeared larger than the right one.
Congenital anomalies of the kidney and the urinary tract (CAKUTs) appear because of the abnormal renal developmental processes, and the incidence is reported to be 1.6 in 1000 births.1 Renal duplication, which is the most common CAKUT, can be complete or partial.2 Two renal pelvises and ureters are formed in complete duplication, whereas partial duplication has two renal pelvises and only one or two ureters that join before connecting to the bladder. CAKUT is often accompanied by vesicoureteral reflux, which is thought to correlate with severe and recurrent urinary tract infections. Complete renal duplication and ureteropelvic junction stenosis have high incidence of vesicoureteral reflux.3 To the best of our knowledge, this is the first report of AFBN with partial renal duplication. The correlation between AFBN and renal duplication cannot be determined only from this case report. In general, asymptomatic partial renal duplication found incidentally does not require further intervention. However, patients with partial duplication might acquire urinary tract infections due to reflux from one renal pelvis to another or stagnation of urine.4 Enlarged kidney on imaging is one of the important features that aids in the diagnosis of AFBN.5 Both partial duplication and multiple episodes of AFBN might have contributed to enlarged kidney in the present case, as shown by the ultrasound on 6-month follow-up. It is noteworthy that the presence of focal loss of corticomedullary differentiation in sonographic findings may help diagnose AFBN.6 When considering the diagnosis of AFBN for patients with renal duplication and enlarged kidneys, other ultrasonographic findings, such as hypoechoic areas, should not be missed.5
Learning points
Vesicoureteral reflux can cause severe urinary tract infections (ie, acute focal bacterial nephritis (AFBN)) in patients with congenital anomalies, such as complete or partial renal duplication.
Clinicians should look for hypoechoic areas when making the diagnosis of AFBN in patients with renal duplication and enlarged kidneys.
Ethics statements
Patient consent for publication
Acknowledgments
The authors are grateful to Hayato Chikai, MD (Department of Pediatrics, Yaizu City Hospital) for his clinical care and treatment of the patient.
Footnotes
Contributors KW, HK and HI managed the patient, drafted the article and revised the final version. TK critically reviewed the manuscript and supervised the whole study process. All authors approved the final manuscript for submission.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.