Article Text

Statistics from Altmetric.com
Description
A 58-year-old man, awaiting lung transplantation, was admitted to our hospital with severe acute exacerbation of chronic obstructive pulmonary disease (COPD). He had been treated with supplemental oxygen and domiciliary nocturnal non-invasive ventilation (NIV) for several years. At admission, standard therapy including systemic corticosteroids and tazobactam/piperacillin was administered. In addition, he was initiated onto the use of inhaled tiotropium/olodaterol, and the NIV was extended to 24 hours a day. However, his dyspnoea did not improve. Morphine hydrochloride (5 mg orally) was then administered to improve the severe dyspnoea. Within 10 min of taking the oral morphine, his respiratory rate had decreased from 23/min to 13/min, and the wheezing had resolved. His dyspnoea was completely relieved 20 min after taking the oral morphine. The logged data on the NIV shortly before taking the morphine revealed tachypnoea (25/min) accompanied by intense inspiratory effort (figure 1, arrow) and below zero expiratory flow before the next inspiration (figure 1, arrow head). This denoted intrinsic positive end-expiratory pressure. Twenty minutes after taking the morphine, the logged data showed improved tachypnoea (15/min), an expiratory flow that had reached zero before expiration ended (figure 2, arrow head) and sufficient inspiratory time (figure 2, arrow). Arterial blood gas analysis was performed while breathing O2 at 1 L/min through nasal prongs before taking oral morphine and was as follows: pH 7.31, PaCO2 56.3 mm Hg and PaO2 89 mm Hg. These values while breathing the same amount of oxygen through nasal prongs improved the next day and were as follows: pH 7.35, PaCO2 53.8 mm Hg and PaO2 112 mm Hg. Oral morphine 10 mg/day was continued for 8 days and then reduced to 5 mg/day for 3 days. Morphine was then discontinued safely and the patient was discharged 2 weeks after discontinuation.

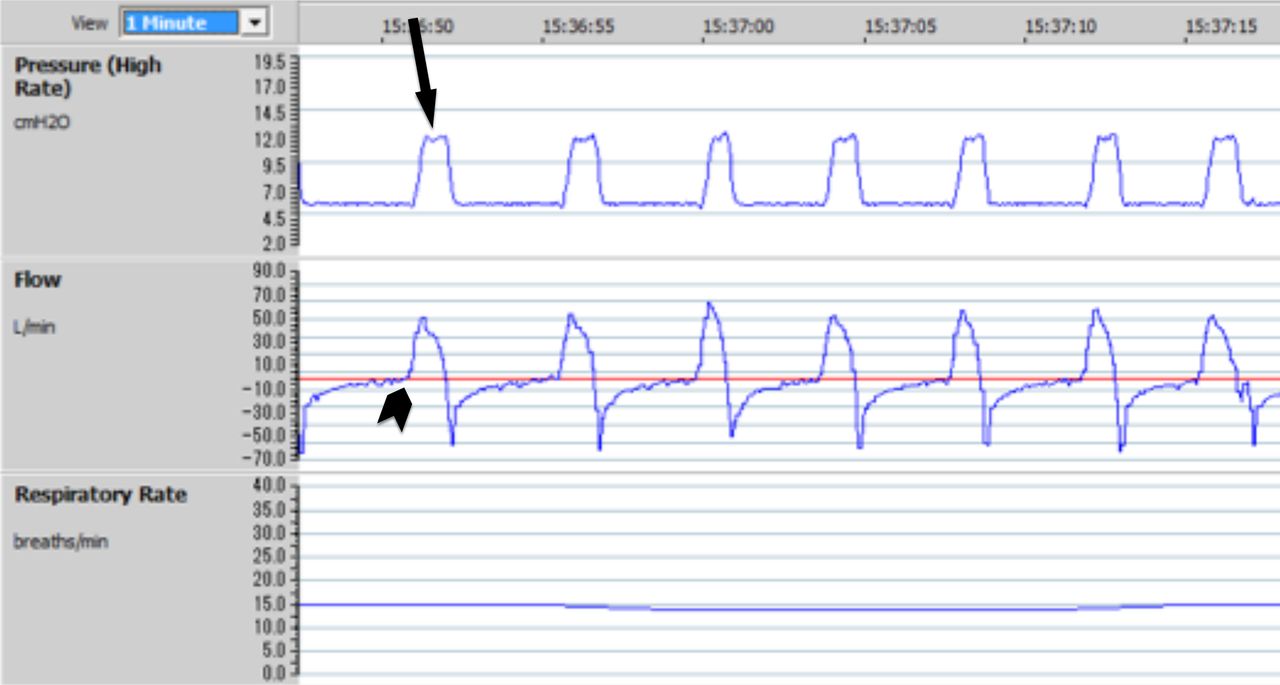
Logged data on the non-invasive ventilation shortly before taking the morphine revealed tachypnoea (25/min) accompanied by intense inspiratory effort (arrow) and below zero expiratory flow before the next inspiration (arrow head).

{kind=link}
{kind=link}
Logged data on the non-invasive ventilation 20 min after taking the morphine showing improved tachypnoea (15/min), an expiratory flow that had reached zero before expiration ended (arrow head) and sufficient inspiratory time (arrow).
Oral morphine is the most commonly prescribed opioids for dyspnoea. Opioids may have multiple mechanisms of action, including reducing ventilation and oxygen consumption, increasing sensitivity to hypercapnia, and reducing the central perception of dyspnoea and anxiety-associated dyspnoea.1 NIV is used to provide relief from dyspnoea.2 In the present case, the inspiratory and expiratory positive airway pressures were set at 12 cmH2O and 6 cmH2O, respectively, in the spontaneous mode. Higher pressures, which may have improved the patient’s ventilation and dyspnoea, could not be tolerated because of pain and oppressive feeling by the higher pressures. The problem with opioids is that they are mostly evaluated subjectively by tools such as the symptom scale. This report highlights the advantage of using logged NIV data as an objective way of monitoring the effect of morphine in acute exacerbations of COPD, as described here.
Learning points
The problem with opioids for refractory dyspnoea is that they are mostly evaluated subjectively by tools such as the symptom scale.
This report highlights the advantage of using logged non-invasive ventilation data as an objective way of monitoring the effect of morphine on dyspnoea in a patient with acute exacerbations of chronic obstructive pulmonary disease.
Ethics statements
Patient consent for publication
Footnotes
Contributors TK: literature search, data collection, analysis of data and manuscript preparation. SY: review of manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.