Article Text

Abstract
Acute pancreatitis (AP) is an acute destructive inflammatory condition of the pancreas. Hypertriglyceridaemia is the third most common worldwide cause of AP. Although the presentation of hypertriglyceridaemic pancreatitis (HTGP) is usually similar to other forms of AP, it may cause more severe AP and worse symptoms. Therefore, apart from the supportive care and treatment for AP, it is necessary to treat the underlying aetiology. There are no established guidelines for managing HTGP. Many treatment modalities have been reported, including intravenous insulin infusion, heparin and plasmapheresis. Randomised trials comparing their efficacy are lacking. Diabetic ketoacidosis (DKA) may be a risk factor for AP, but it is uncertain if AP triggers DKA or vice versa. Here, we describe a case of a 44-year-old man who presented with DKA concurrent with acute severe HTGP as first manifestation of type 2 diabetes mellitus. He was successfully managed with supportive care and intravenous insulin infusion.
- pancreatitis
- diabetes
- lipid disorders
- metabolic disorders
- adult intensive care
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Acute pancreatitis (AP) is a common and acute destructive inflammatory condition of the pancreas. It is characterised by abdominal pain and elevated levels of pancreatic enzymes in the blood. Hypertriglyceridaemia (HTG) is the third most common worldwide cause of AP after gallstones and alcohol.1 Although the clinical presentation of hypertriglyceridaemic pancreatitis (HTGP) is usually similar to other forms of AP, it may cause more severe AP and worse symptoms.2 HTG is considered a significant risk for AP when its levels are >11.3 mmol/L (1000.9 mg/dL). As triglyceride levels increase, the incidence of AP also increases.3 4 The initial management plan of patients with HTGP includes supportive care and treatment of AP, such as fluid resuscitation, pain control and nutritional support. Additional therapy to reduce the serum triglyceride levels is also very important to prevent life-threatening complications. There are no established guidelines for managing HTGP. Insulin therapy has previously been used in these patients with promising outcomes.5
Case presentation
A 44 -year-old man presented to our emergency department (ED) on 10 March 2020 with constant upper abdominal pain for 8 days. The pain radiated to the back for 3 days and was accompanied by anorexia and nausea. He was afebrile and denied any other related symptoms. He has a history of arterial hypertension that was well controlled with losartan 50 mg daily and regular follow-up by a general practitioner. He smoked cigarettes for 20 years, about one pack daily. He denied alcohol or illicit drug use. He was married and worked as a chef. His family history was not relevant.
On arrival at the ED, he was alert, oriented and cooperative. His vital signs were: temperature of 37.1°C, blood pressure of 135/74 mm Hg, respiratory rate of 21/min and pulse rate of 98/min. His weight was 79 kg, height 165 cm (body mass index 29 kg/m2). The cardiopulmonary auscultation was normal, abdomen examination revealed tenderness in the epigastric region, no hepatosplenomegaly or masses. Bowel sounds were present and normal. Neurological examination was unremarkable.
The relevant laboratory results at the time of admission are provided in tables 1 and 2. The serum was lipaemic on gross examination as shown in figure 1. Laboratory parameters were remarkable for high anion gap metabolic acidosis with uncompensated respiratory alkalosis, HTG, hyperglycaemia, markedly elevated serum lipase levels and urine ketones positive. Serum electrolytes, liver and renal function tests, coagulation profile and lactate dehydrogenase were within normal limits. Chest X-ray and abdominal X-ray were normal. An abdominal CT was performed and demonstrated an enlargement of the the distal pancreatic body and tail with blurred contour and peripancreatic fluid collection; focal hypodense area was found in the pancreatic tail. These findings were suggestive of AP, with necrosis in the pancreatic tail (figure 2). There was no evidence of gallstones.

The blood sample was lipaemic on gross examination.

CT abdomen showing the distal pancreatic body and tail are enlarged with blurred contour and peripancreatic fluid collection. A focal hypodense area is found in the pancreatic tail (arrows). Acute pancreatitis with necrosis in the pancreatic tail is suggested.
Initial laboratory results of the patient with respective reference ranges.
Initial arterial blood gas results of the patient with respective reference ranges.
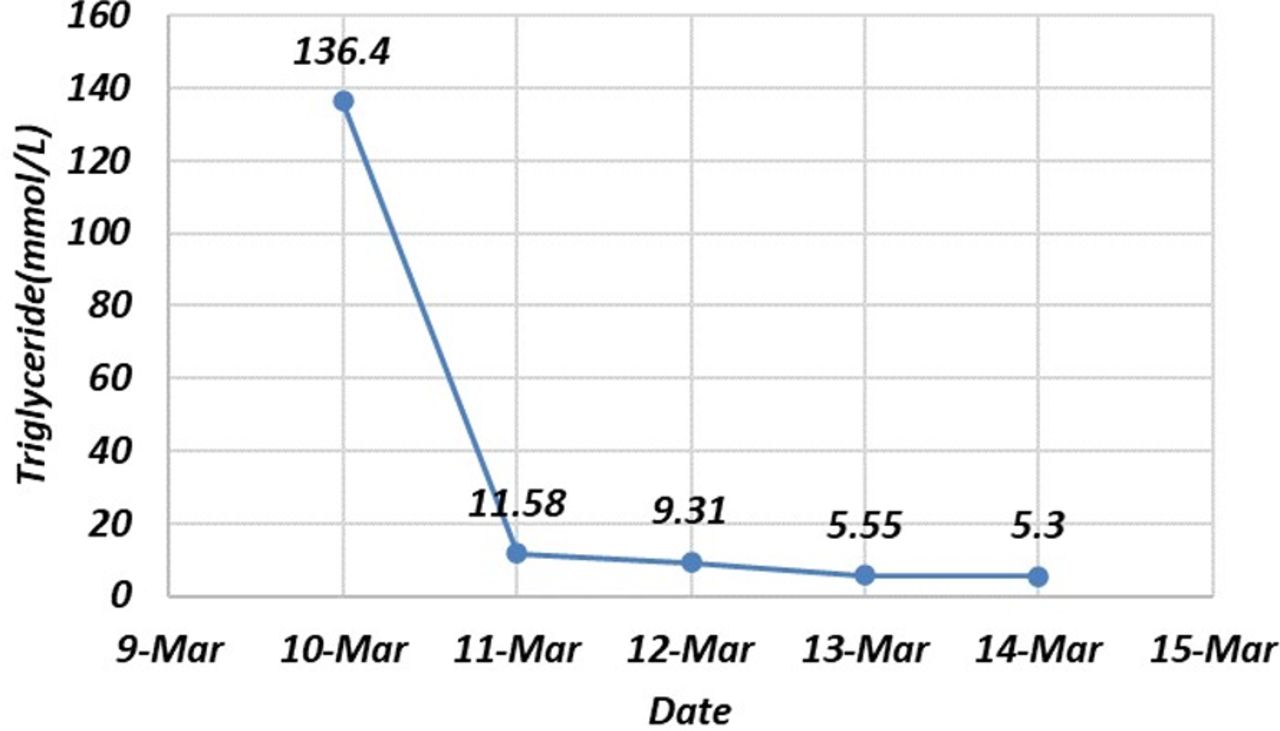
Based on the evidence of the clinical findings, laboratory and radiological investigations, the patient was diagnosed with HTGP and diabetic ketoacidosis (DKA). Thus, he was admitted to the medical intensive care unit for fluid resuscitation, pain control, bowel rest and intravenous insulin infusion therapy for both HTGP and DKA. The intravenous insulin infusion regimen we used was the DKA insulin therapy protocol. The insulin infusion was initiated at a rate of 0.1 units/kg/hour and was titrated for target a reduction of capillary blood glucose by 3.0 mmol/L/hour, a rise of the venous bicarbonate by 3.0 mmol/L/hour and a maintenance of serum potassium between 4.0 and 5.5 mEq/L. After 1 day of intravenous insulin infusion therapy, his metabolic acidosis resolved and triglyceride level downtrended from 136.4 mmol/L to 11.58 mmol/L (12081 mg/dL to 1025.7 mg/dL). The intravenous insulin infusion therapy with 5% dextrose was continued with monitoring serum glucose every 1–2 hours, triglyceride every 24 hours and electrolytes monitoring every 12 hours. The insulin infusion therapy was stopped on day 4 when there was clinical improvement and the triglyceride level had decreased to 5.3 mmol/L (469.4 mg/dL) (figure 3).
{kind=link}
{kind=link}
{kind=link}
Curve indicating the changes in serum triglyceride levels during intravenous insulin infusion therapy.
Outcome and follow-up
He was transferred from the medical intensive care unit to the general surgical ward after clinical improvement. He resumed oral feeding that was well tolerated. He was started on atorvastatin 40 mg daily, fenofibrate 160 mg daily and insulin therapy for diabetes and hyperlipidaemia control. He was discharged to follow-up by internal medicine consultation. At the 1-month follow-up, the patient showed complete recovery of the symptoms with serum triglyceride level decreased to 3.37 mmol/L (298.5 mg/dL). The control abdominal CT showed improvement of the distal pancreatic body and tail findings, and decrease in the volume of the peripancreatic fluid collection compared with the initial CT study. No new lesion was found in the pancreas and the peripancreatic region. At the 4-month follow-up, the patient’s serum triglyceride level decreased to 2.53 mmol/L (223.89 mg/dL) and haemoglobin A1c (HbA1c) to 12.9%. His glycaemia is being controlled with diet control, Humalog Mix (mixture of insulin lispro and insulin lispro protamine), metformin and empagliflozine, still under adjustment for better diabetes and hyperlipidaemia control. His insulin and C peptide level were normal. Unfortunately, the patient has missed follow-up for several months already.
Discussion
AP is an inflammatory condition of the pancreas characterised by abdominal pain and elevated levels of pancreatic enzymes in the blood. Pancreatic duct and acinar injuries, by direct or indirect toxicity, impaired secretion and premature activation of digestive enzymes leading to autodigestion and acute inflammation. HTG is an important cause of acute AP.1 HTGP may cause more severe AP and worse symptoms.2 Thus, early clinical recognition of HTGP is important to provide appropriate therapy. The exact pathogenesis of HTGP is not fully understood. However, there have been a number of hypothesis relating to HTG. Triglycerides themselves do not appear to be toxic. The excess of triglycerides are subsequently hydrolysed by pancreatic lipases to release free fatty acids (FFAs). This releases high levels of FFAs that exceed the binding capacity of plasma albumin. These unbound FFAs self-aggregate into micellar structures with detergent properties. These toxic structures can cause damage to platelets, vascular endothelium and acinar cells, which result in ischaemia and acidosis which further worsens the FFA toxicity.6 7 Furthermore, excess serum triglycerides also increase the blood viscosity. Hyperviscosity leads to capillary plugging and impairs the vascular flow to the pancreas. This blockage can also increase the acidity of the pancreas, which predisposes the pancreas to acute inflammation through activation of trypsinogen.6 7
The diagnosis of HTGP is the same as other aetiologies of AP, which is based on the revised Atlanta classification criteria—presence of two of the following three criteria: (1) acute onset of persistent, severe epigastric pain often radiating to the back, (2) elevation in serum lipase or amylase to three times or greater than the upper limit of normal, and (3) characteristic findings of AP on imaging (contrast-enhanced CT, MRI or transabdominal ultrasonography).8 It can be difficult to identify HTG as the aetiology in AP. HTGP should be suspected in patients with AP and risk factors for HTG. Risk factors include poorly controlled diabetes, alcoholism, obesity, pregnancy, prior pancreatitis and a personal or family history of HTG.9–12 Serum triglyceride levels >11.2 mmol/L (992 mg/dL) are required for HTG to be considered the underlying aetiology of AP.3
DKA may be a risk factor for AP, but it is uncertain if AP triggers DKA or vice versa. In patients with type 1 diabetes, decreased insulin production results in a marked reduction in lipoprotein lipase activity, which leads to HTG. Hyperinsulinaemia and insulin resistance in patients with type 2 diabetes enhances triglyceride production and decreases plasma triglyceride clearance.10 On the contrary, HTGP results in acute beta cell dysfunction, causing transient insulin deficiency and also increase in insulin resistance due to systemic inflammation, thus possibly triggering DKA.13 In our case report, the patient had annual check-up in a private clinic and had no previous history of dyslipidaemia. His initial blood test showed highly elevated HbA1c (13.1%, normal range 4.0%–6.0%). Thus, DKA was considered to be the primary trigger.
There are no established guidelines for managing HTGP. The initial treatment should adhere to the practice recommendations as established for AP, including fluid resuscitation, analgesic treatment and bowel rest. Following this initial conservative management, it is necessary to rapidly reduce the level of serum triglycerides. Many treatment modalities have been reported, including intravenous insulin infusion, heparin and plasmapheresis. Randomised trials comparing their efficacy are lacking. Intravenous insulin infusion therapy has previously been used in these patients with promising outcomes to decrease serum triglyceride.5 The mechanism by which insulin lowers the level of serum triglycerides is by enhancing lipoprotein lipase activity, an enzyme that accelerates chylomicron and very low-density lipoprotein metabolism to glycerol and FFAs.14 15 Therefore, it ultimately decreases the serum triglyceride levels. Because HTGP often presents in patients with uncontrolled diabetes, insulin can concurrently control hyperglycaemia in these patients. Studies have reported that insulin therapy can lower triglyceride levels to less than 5.6 mmol/L (496 mg/dL) over 3–4 days.16 17 Alternatively, in patients with HTGP presenting with one or more worrisome features, such as signs of hypocalcaemia, lactic acidosis, signs of worsening systemic inflammation or signs of worsening organ dysfunction or multiorgan failure, initial therapy with therapeutic plasma exchange is recommended.18
Conclusion
The presentation of DKA concurrent with acutely severe HTGP as first presentation of type 2 diabetes mellitus is extremely rare. There is no established guideline for the treatment of HTGP. In our case, we successfully managed acutely severe HTGP while treating DKA with intravenous insulin infusion as reported by other authors, supporting once more the safety of this therapeutic option.
Learning points
Diabetic ketoacidosis (DKA) may be a risk factor for acute pancreatitis (AP), but it is uncertain if AP triggers DKA or vice versa.
Hypertriglyceridaemic pancreatitis (HTGP) may cause more severe AP and worse symptoms. Rapidly reducing the level of serum triglycerides is important.
Intravenous insulin infusion therapy is a safe and effective treatment option with promising outcomes in controlling acutely severe HTGP while treating DKA.
Acknowledgments
We would like to express our grattitude to Dr. Ng Hou, Chief Doctor of Internal Medicine Department for his support. Assistance provided by Dr. Alberto Mello e Silva was greatly appreciated.
References
Footnotes
Contributors Dr Man Tek Kong took care of the patient during his admission in the Intensive Care Unit and is the lead author of this case report.
Dr Monica Pon follows up and treats the patient in Internal Medicine outpatient department. She gave guidance to write the case report and is the correspondance author of this case report.
Dr Kan Fat Leong was the responsible doctor during the patient’s admission in the Intensive Care Unit.
Dr Hou Ng is the chief physician of Internal Medicine.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer-reviewed.