Article Text

Statistics from Altmetric.com
Description
Re-expansion Pulmonary oedema (RPE) is a rare but potentially fatal complication, which can arise after a rapid decompressive treatment of pulmonary collapse secondary to pleural effusion, pneumothorax or atelectasis. The pathophysiological mechanism is still poorly understood, admitting a multifactorial aetiology underlying the process of increasing the permeability of the pulmonary microvascular structure secondary to the abrupt re-expansion process.1 2
A 21-year-old male patient, active smoker (three pack-years), without drug abuse, recent trauma or pathological history. He was admitted to the emergency department after 6 days of sudden onset of dyspnoea, left pleuritic chest pain, palpitations and dry cough, with progressive worsening.
The patient had no evident morphological abnormalities, blood pressure was 112/68 mm Hg, heart rate 100 bpm, respiratory rate 22 bpm, peripheral oxygen saturation of 99% (room air) and was apyretic. He presented a hyper-resonant left haemithorax with decreased lung sounds on auscultation. Chest X-ray confirmed left tension pneumothorax (figure 1). Blood samples showed normal haemogram, coagulation and inflammatory parameters. The patient was then treated with oxygen therapy and placement of a chest tube on the fifth left intercostal space, with subaquatic seal (without suction), leading to improved symptoms.
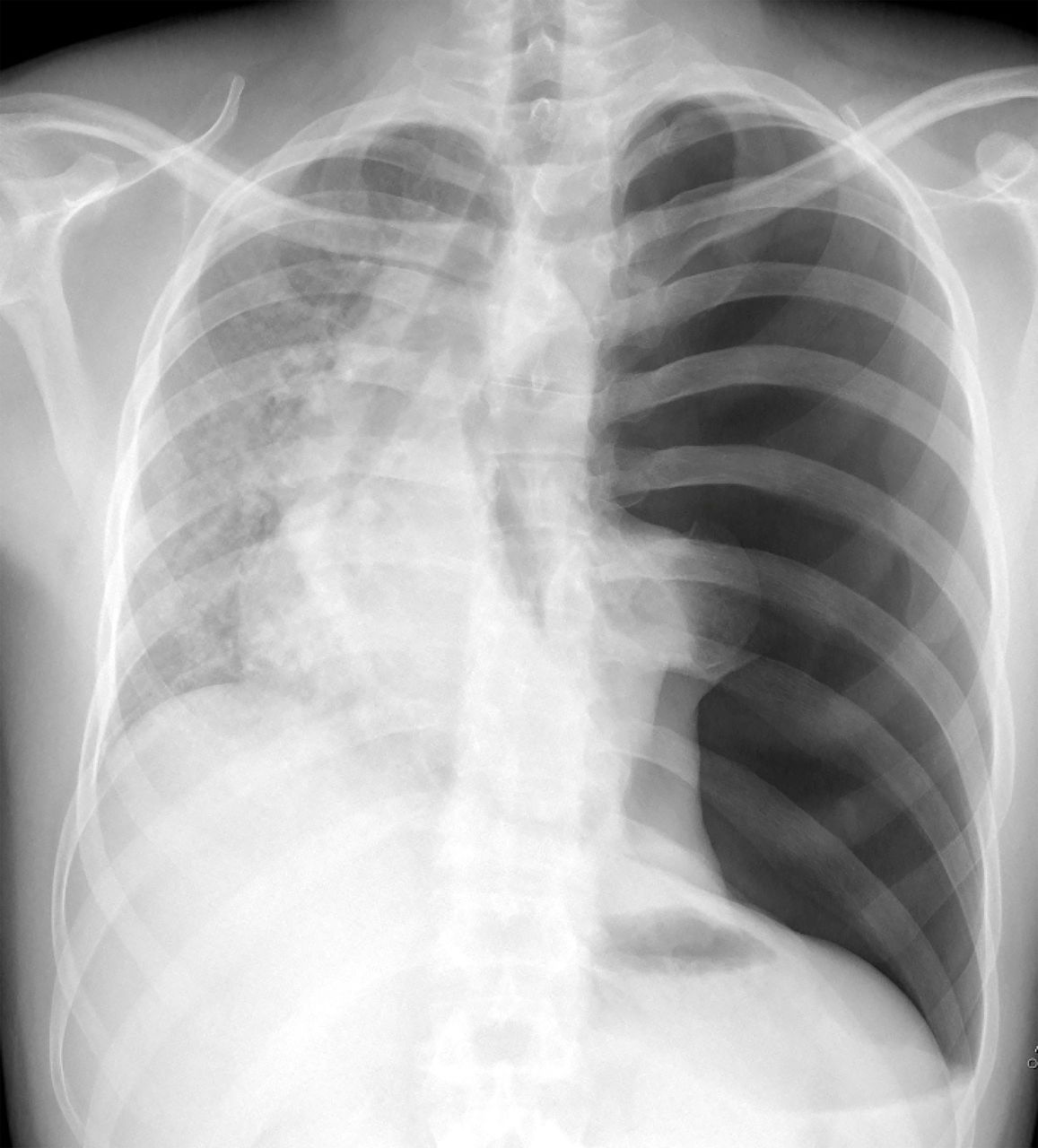
Chest X-ray showing complete left lung collapse, tracheal and mediastinal deviation to the right side.
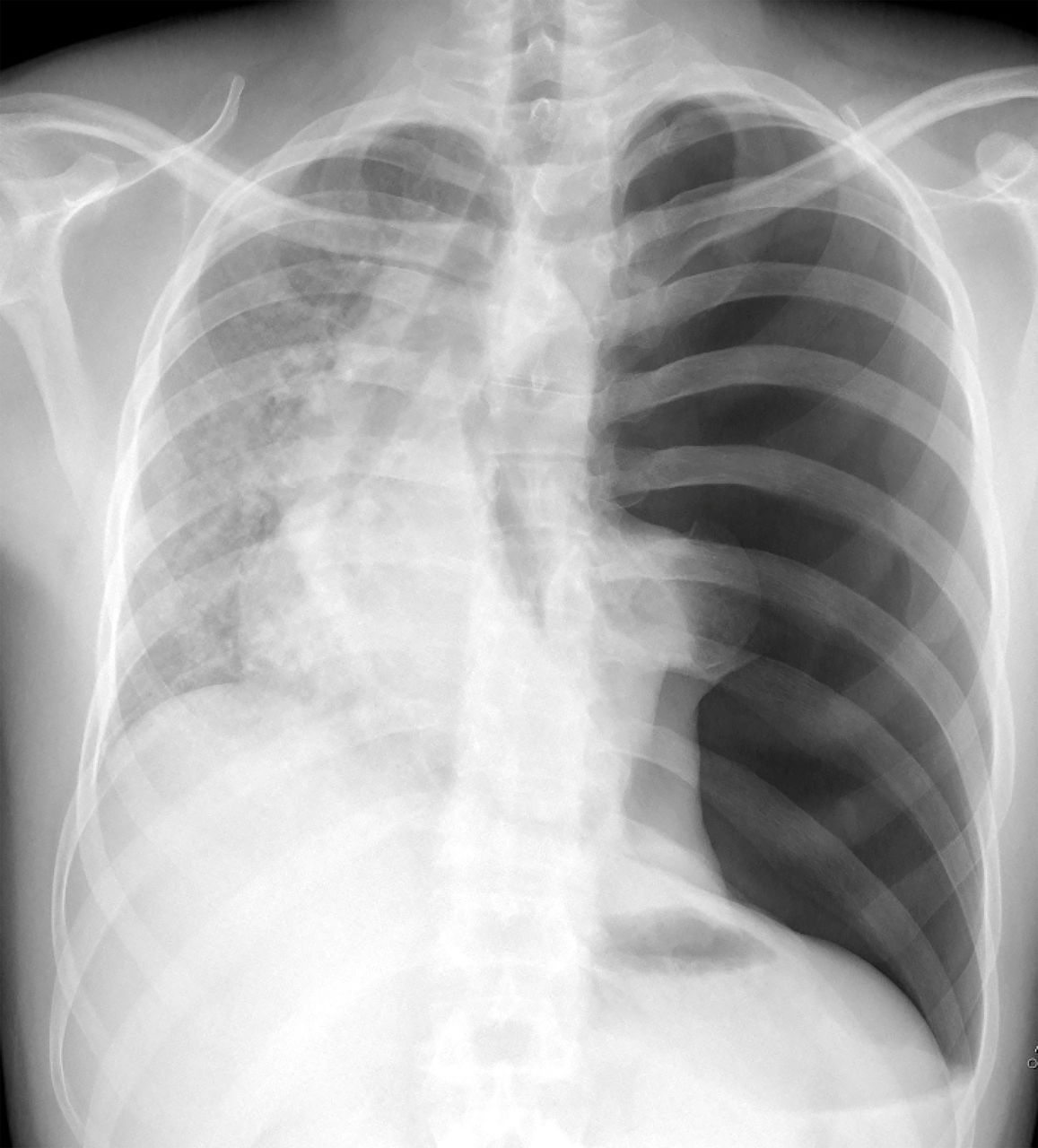
One hour after the procedure he developed tachycardia, productive cough, dyspnoea and respiratory distress, unresponsive to oxygen therapy. A repeat chest X-ray confirmed the correctly positioned chest tube, complete left lung expansion, but showed alveolar opacities (figure 2). RPE was assumed and treatment with diuretics, corticosteroids and continuous positive airway pressure was initiated. As a result, the symptoms improved, and clinical stability was achieved.

{kind=link}
{kind=link}
Chest X-ray showing alveolar opacities on the left lung, chest drainage tube with extremity positioned on the left lung apex.
The patient was transferred to intermediate care unit and positive pressure was stopped. One hour after, he underwent in to acute respiratory failure, requiring orotracheal intubation, invasive mechanical ventilation and admission into intensive care unit. He stayed on mechanical invasive ventilation for 6 days. At the 7th day of intensive care unit stay, there was a complete resolution of RPE, but a persistent air leak was noted, so the patient was submitted to surgical pleurodesis (pleural abrasion) via video-assisted-thoracoscopy. He was discharged 10 days later, asymptomatic and with a normal chest X-ray.
The diagnosis of RPE is made by a combination of clinic and imaging findings. Most common symptoms include productive cough, tachycardia, hypotension, cyanosis, fever and chest pain. The severity of the symptoms is variable, from mild (documented only by imaging), to acute respiratory distress syndrome. The most common finding in chest X-rays is an alveolar filling pattern, usually ipsilateral but it can reach any anatomical portion of the lung parenchyma. These findings usually arise between 2 and 4 hours after the thoracic cavity drainage, which can worsen in the first 48 hours and persist for four to 5 days, after which the oedema is expected to resolve, typically without sequelae.3–5
Stablished RPE risk factors include longer pneumothorax evolution, usually greater than 3 days and pneumothorax size, being the risk directly proportional to its size. It is usually a self-limiting complication that only requires supportive treatment, with oxygen therapy, diuretics and positive pressure therapy. In greater severity situations, systemic corticosteroid therapy is advised and invasive mechanical ventilation may be necessary.3 5 6
Learning points
Re-expansion pulmonary oedema can arise after a rapid decompressive treatment of the pneumothorax.
The risk of occurrence increases with the pneumothorax duration and its size (increased risk for larger pneumothorax).
Treatment is supportive care, but steroids, haemodynamic and ventilatory support may be needed.
Ethics statements
Patient consent for publication
Footnotes
Contributors Substantial contributions to the conception or design of the work, or the acquisition, analysis or interpretation of data: DR, MV and TC. Drafting the work or revising it critically for important intellectual content: DR, MV and TC. Final approval of the version published: DR, MV and TC. Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved: DR, MV and TC.
Funding This study was funded by Centro Hospitalar e Universitário de Coimbra (945074).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.