Article Text

Statistics from Altmetric.com
Description
Aortic intramural haematoma (IMH) is an acute aortic syndrome which constitutes 5%–20% of all acute aortic syndromes.1 It is defined as a contained haemorrhage into the media without rupture of the intima.2 It is thought to either be due to rupture from a penetrating atherosclerotic ulcer that then thromboses the false lumen or due to spontaneous rupture of a vasa vasorum. IMH has been reported to progress to acute aortic dissection in up to 88% of patients when the ascending aorta is involved.3 IMH also has a higher risk of aortic rupture than aortic dissection due to the outer media being thinner. We present a case where aortic IMH was initially suspected on coronary angiography and subsequently confirmed on ancillary imaging.
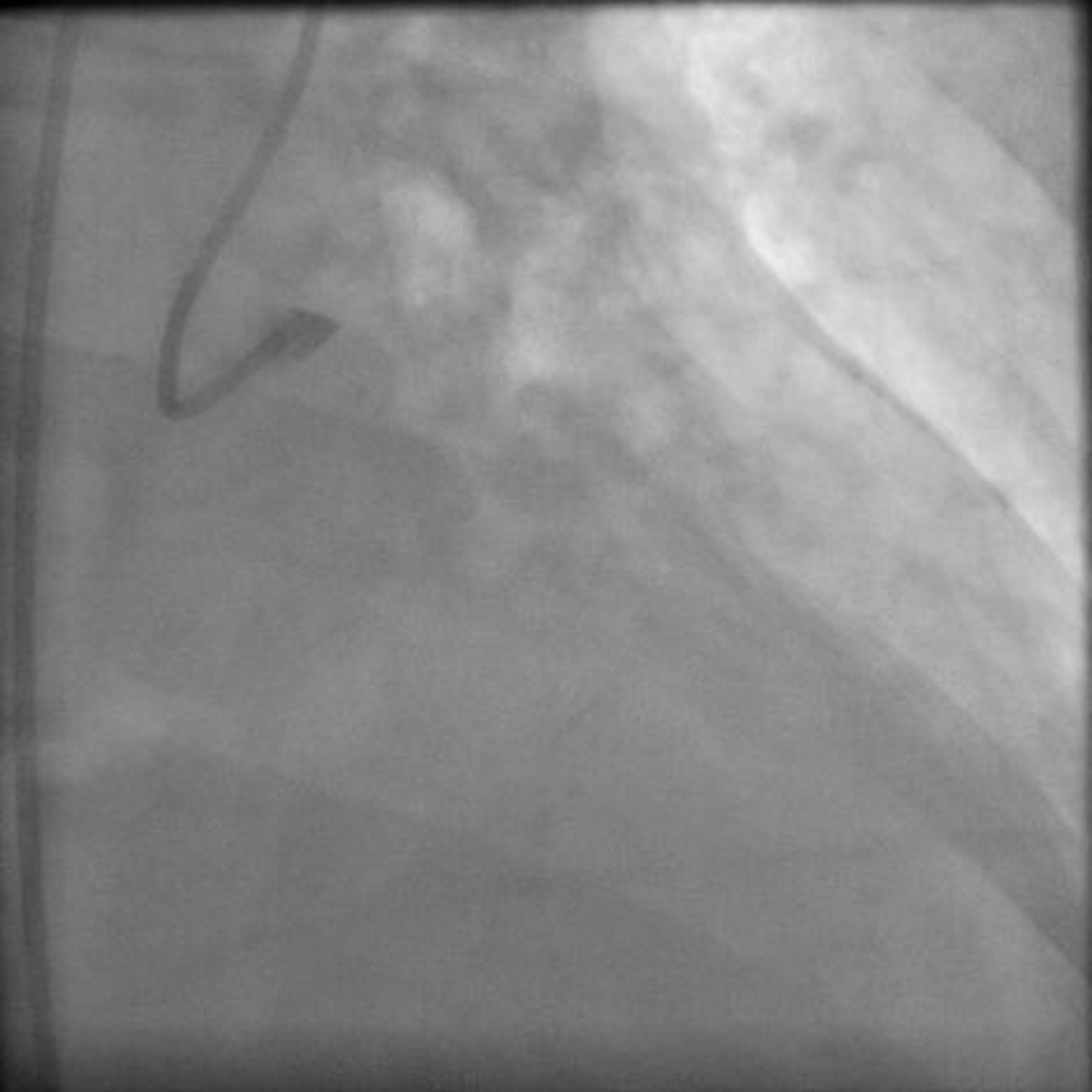
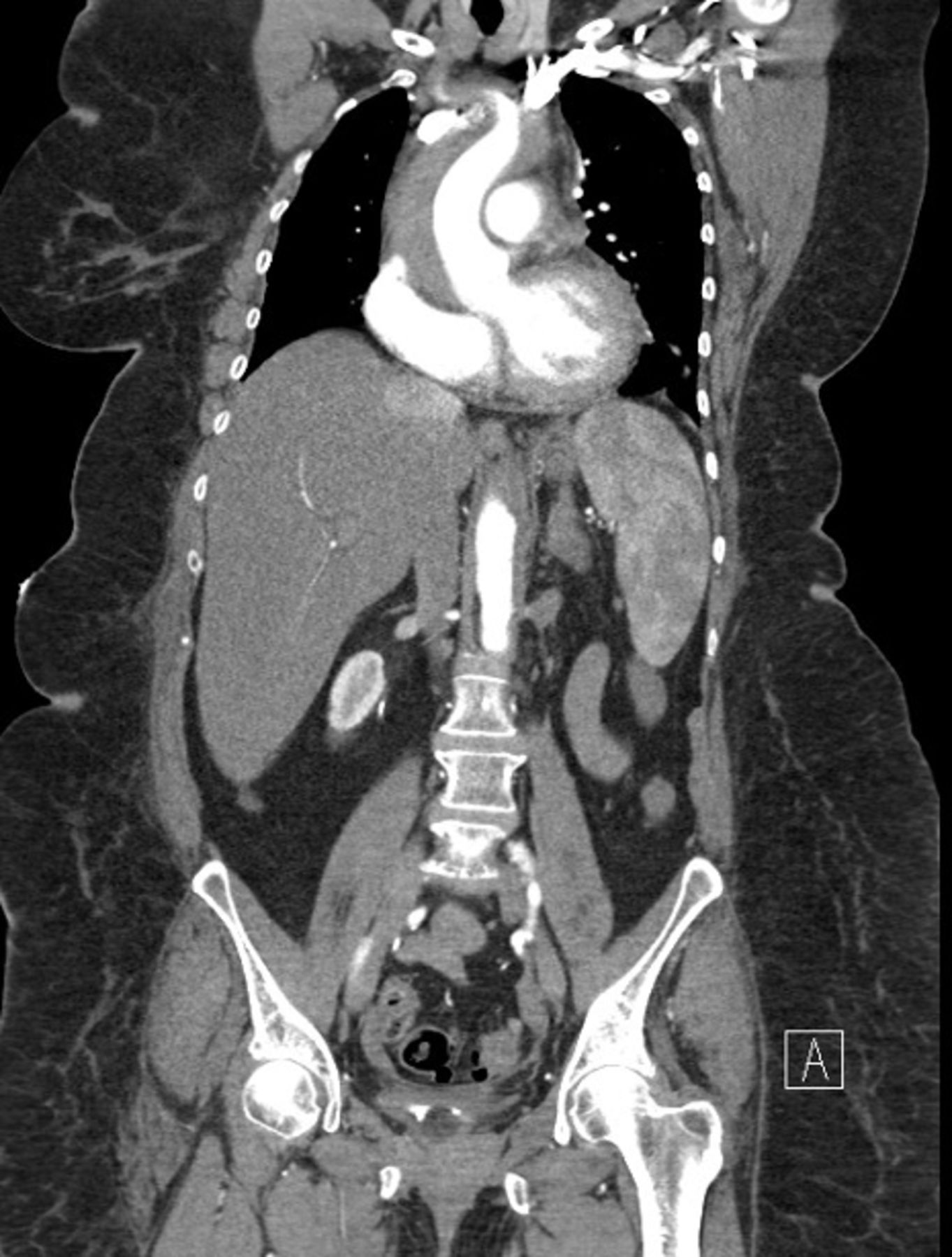
A 61-year-old woman with a history of hypertension, hyperlipidaemia, type 2 diabetes, previous non-ST elevation myocardial infarction and previous smoking presented to a rural emergency department (ED) with atypical chest pain. Her vital signs in the ED were a heart rate of 55, right arm blood pressure of 118/57, left arm blood pressure of 115/54, oxygen saturation of 95% on 2-litre nasal prongs and a temperature of 36.4°C. ECG revealed sinus bradycardia with old inferior q-waves and lateral ST-depression and her troponin I was elevated at 0.10. Chest X-ray was not of good quality to evaluate the mediastinum (online supplemental figure 1). Unfortunately, a d-dimer was not measured at the rural ED and a bedside echocardiogram was unavailable. The patient was therefore treated as a non-ST elevation myocardial infarction transferred for angiography. Coronary angiography revealed no obstructive coronary artery disease, however, initial left coronary artery engagement was suspicious for a possible penetrating atherosclerotic ulcer (figure 1). Root aortogram was performed, which revealed no evidence of dissection. Given this, the patient went on to have a CT angiogram of the chest which revealed a large type A IMH extending from the aortic root to the level of the left renal artery (figure 2).
Supplemental material

Coronary angiography with injection into penetrating atherosclerotic ulcer.

{kind=link}
{kind=link}
CT Angiogram Coronal View Demonstrating Type A IMH Extending from the Aortic Root.
The patient was subsequently taken for emergent aortic repair. Intraoperatively she had significant bleeding and left main coronary button failure requiring coronary artery bypass grafting. Postoperatively she developed multiorgan failure and died on post-operative day 3.
Learning points
Aortic intramural haematomas are associated with penetrating atherosclerotic ulcers.
D-dimer should be considered in patients presenting with chest pain to rule-out causes such as aortic dissection/haematoma and pulmonary embolism.
Aortic intramural haematomas may not be associated with a widened mediastinum on chest X-ray and may have a normal aortic root shot on coronary angiography.
Bedside echocardiogram should be considered in chest pain/troponin elevation presentations to identify regional wall motion abnormalities as well as non-coronary pathologies such as aortic dissections/intramural haematomas.
Ethics statements
Patient consent for publication
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @arkugu21
Contributors AKG and JMS both examined and treated the patient. AKG and JMS shared equal parts in the writing and preparation of the manuscript. Both authors approve it for publication.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.