Article Text

Abstract
Little is known about sleep-based approaches to the treatment of nocturnal enuresis (NE). This report is the first to describe the successful use of suvorexant, an orexin receptor antagonist, in a 12-year-old boy with intractable NE. With suvorexant, the frequency of NE gradually decreased from 14 of 14 days (100%) to 5 of 14 days (35.7%). Sleep polysomnography indicated that rapid eye movement (REM) sleep increased from 101.5 min (19.9%) before suvorexant to 122.1 min (24.9%) with suvorexant. Furthermore, N2 increased from 233 min (45.6%) to 287.5 min (58.7%) during non-REM sleep. In contrast, N3 decreased from 160 min (31.3%) to 65 min (13.3%) during non-REM sleep. Suvorexant appeared to lighten the depth of sleep and alter sleep architecture. Although the application of an insomnia medication for treating NE seems paradoxical, suvorexant reduced the frequency of NE in patients with severe intractable NE. Thus, this treatment strategy warrants further examination.
- paediatrics
- urology
- sleep disorders
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
In recent years, several therapies based on International Children’s Continence Society recommendations have been used to treat nocturnal enuresis (NE). However, some children are resistant to current treatments. It is estimated that 2.02% of 12-year olds will experience NE.1 This is a particularly serious problem for children who continue to have NE afterwards. The present article focuses on depth of sleep as a cause of NE that is not yet fully understood and considers whether it might lead to new treatment options.
Several reports have examined sleep depth and sleep architecture in individuals with NE because these may be important factors associated with this condition.2–4 Many children with NE have difficulty awakening from sleep compared with those without NE.3 Children with NE are generally believed to be deep sleepers with impaired arousability.2 However, recent studies using all-night electroencephalography or biomotion sensors have shown that children with NE are relatively light sleepers.4 5 To date, no reports have described a sleep-based approach to treating NE that led to the successful reduction of NE frequency. In this report, the role of sleep depth was examined in a patient with intractable NE. Intractable NE was defined as that which could not be effectively treated with behaviour modification, desmopressin, an enuresis alarm, anticholinergics, tricyclic antidepressants or other interventions considered to be gold standard treatments.
Psychoactive drugs such as diazepam were once used to treat NE because they alter sleep levels.6 7
In a recent study, sleep in monkeys who had been given orexin receptor antagonists resembled sleep without drugs, and arousal from sleep via acoustic stimuli was maintained along with the underlying sleep architecture. In contrast, while diazepam induced light sleep, the monkeys rarely woke up in response to salient stimuli.8 This suggests that standard insomnia medications might not be appropriate for patients with NE because they can decrease wakefulness at night and may decrease inhibition of urination during sleep, thus increasing the frequency of NE.
Suvorexant is an orexin receptor antagonist that was newly developed for the treatment of insomnia. Sleep polysomnography has indicated that it can increase both N2 and rapid eye movement (REM) sleep.9 While benzodiazepines (BZDs) and non-BZD hypnotics that act on gamma-aminobutyric acid (GABA) induce a nonphysiological deep sleep, suvorexant has a completely different mechanism for treating insomnia. Specifically, it promotes the natural transition from wakefulness to sleep by inhibiting orexin neurons that promote wakefulness in the arousal system. Furthermore, it induces physiological sleep that is not excessively deep compared with conventional sleep-inducing drugs.10 In other words, suvorexant inactivates wakefulness rather than promoting sleep. This suggests that suvorexant may be useful in treating patients with NE caused by excessively deep sleep.
Suvorexant may help treatment-resistant children with NE engage in relatively lighter sleep, thereby enabling them to inhibit urination or to help them awaken when they feel the need to urinate.
Case presentation
This is the first report of the successful use of suvorexant to reduce the frequency of NE in a patient with intractable NE. The patient was a 12-year-old boy with normal growth and development, no learning difficulties, no attention-deficit/hyperactivity disorder, no family problems, normal renal function, normal bladder capacity, and no family history of NE.
The child had no underlying diseases, and no history of any sleep-related disorders or factors such as obstructive sleep apnea.
Daytime toilet training was completed at 3 years of age, and since then, no daytime incontinence occurred. The patient was able to control his urination while awake. He was diagnosed with primary monosymptomatic NE. Prior to the administration of suvorexant, the patient had already been treated with behaviour modification, desmopressin, an enuresis alarm, anticholinergics, tricyclic antidepressants and traditional Kampo medicine. However, bed-wetting remained continuous until he was 12 years old. All treatment strategies were ineffective and not a single day went by without bed-wetting.
Prior to the administration of suvorexant, the treatment was fully explained to the patient and his parents and informed consent was obtained. At the start of treatment, the author confirmed that the patient was not undergoing any existing treatment for NE.
Treatment
Prior to the start of suvorexant treatment, sleep polysomnography was performed to derive the sleep architecture at baseline (figure 1). Suvorexant (15 mg) was then started with 0.25 tablets once a day before sleep. On the first day after starting suvorexant, the patient reported that the previous night had been the first in his life in which bed-wetting did not occur. The suvorexant dose was then gradually increased to 0.5 and 0.75 tablets at 2-week intervals. When the patient’s body weight reached 40 kg, the dose was increased to one suvorexant (15 mg) tablet as a maintenance dose. Because the tablets were not scored, the correct amount was dispensed using a tablet cutter.
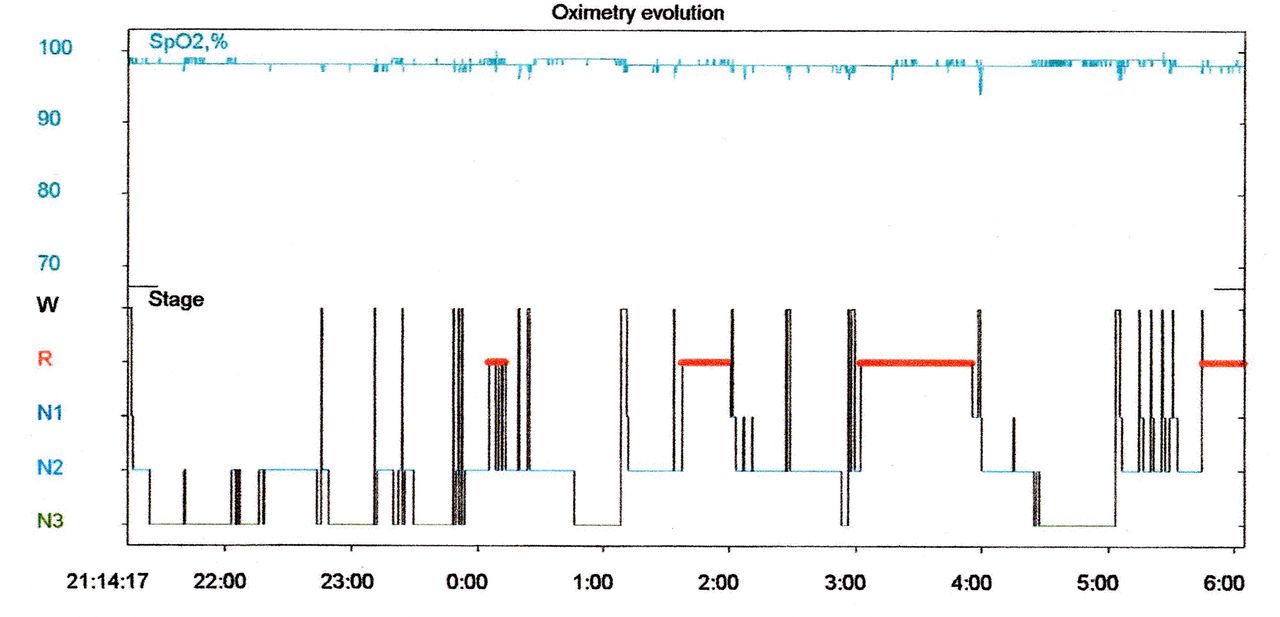
First sleep polysomnography session (before suvorexant treatment).
The drug dosage was increased gradually while monitoring the presence of side effects. Suvorexant was administered in an ‘off-label’ manner because no clinical trials of suvorexant had been conducted in paediatric patients at this time. The patient was started on a very small dose (a quarter of a 15 mg tablet), and a 15 mg tablet is equivalent to a small dose according to Japanese regulations. Depending on the dose, the most commonly reported side effects of suvorexant are somnolence, sedation, muscle weakness, abnormal dreams and headache.10
However, a study on the effects of suvorexant in adolescents between the ages of 10 and 20 suggested that suvorexant was safe and that it could be considered a treatment option for adolescents with insomnia.11
Outcome and follow-up
During the intervention period, the frequency of NE gradually decreased with slight variations and eventually decreased to 5 of 14 days (35.7%).
Afterwards, the rate of NE was maintained such that it occurred on 1 of every 3 days. This result was considered to be the reduction effect of suvorexant on NE. At the point when the frequency of NE had stabilised such that it occurred on 1 of every 3 days, suvorexant was discontinued to confirm whether it had a direct effect on the frequency of NE. After the discontinuation of suvorexant, the frequency of NE increased to 13 of 14 days (92.9%). When the patient resumed suvorexant treatment, the frequency of NE decreased again to 5 out of 14 days (35.7%). Suvorexant was then discontinued again to evaluate the effect of suvorexant on NE, and again the frequency of NE increased to 13 of 14 days (92.9%). Thus, the process of discontinuing suvorexant was repeated two times with the same results.
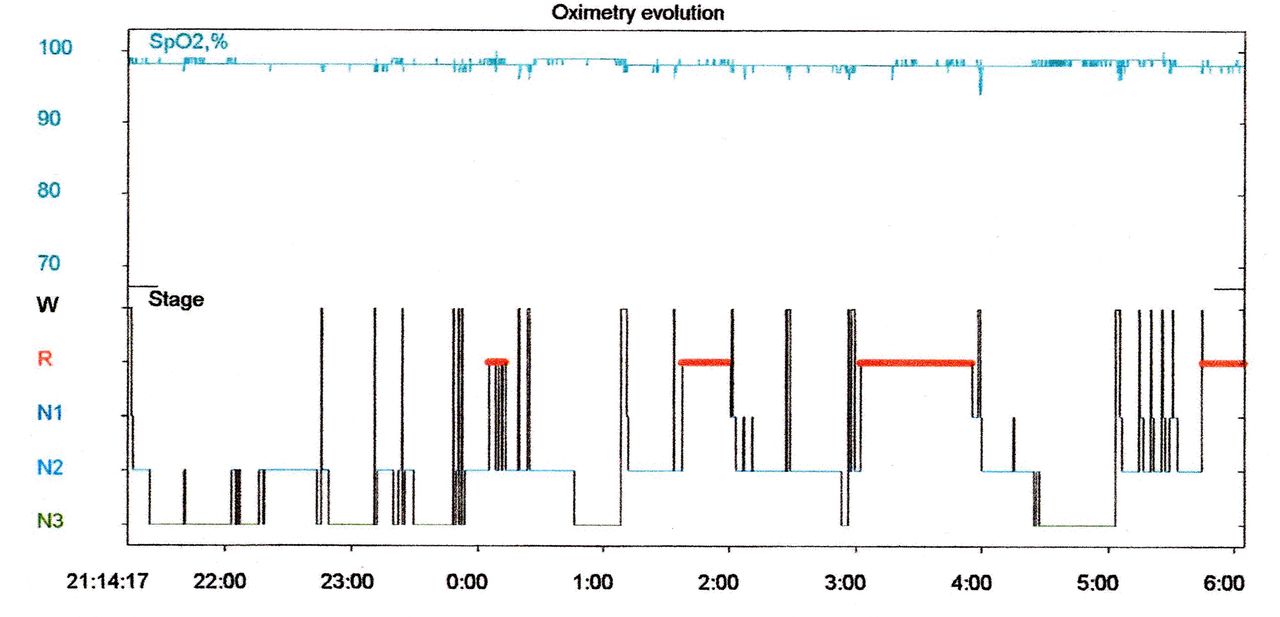
To investigate the effect of suvorexant on sleep, the author performed a second sleep polysomnography session under suvorexant treatment (figure 2). Bed-wetting did not occur during the examination.

{kind=link}
{kind=link}
Second sleep polysomnography session (during suvorexant treatment).
Sleep polysomnography data from before versus during suvorexant treatment were compared (table 1).
Analysis of sleep polysomnography
The total sleep time before versus during suvorexant treatment did not change substantially (from 511 min of sleep before suvorexant to 489.5 min during suvorexant treatment). Before suvorexant treatment, the total amount of non-REM sleep, especially early morning non-REM sleep, was higher. However, overall non-REM sleep decreased after administration, especially early morning non-REM sleep. REM sleep increased from 101.5 min (19.9%) at baseline to 122.1 min (24.9%) with suvorexant, and the length of N2 increased from 233 min (45.6%) to 287.5 min (58.7%) during non-REM sleep. In contrast, N3 decreased from 160 min (31.3%) to 65 min (13.3%) during non-REM sleep. The rate of N1 did not change substantially (from 3.2% before to 3.1% during treatment).
The results indicated that suvorexant administration resulted in lighter sleep architecture.
The patient continued to take suvorexant (15 mg) for 1 year and 4 months after the first dose of suvorexant was started. The reduction in the frequency of NE has persisted.
Discussion
No previous reports have described a successful reduction in the frequency of NE via sleep manipulations. One found that melatonin did not alter NE frequency in patients with therapy-resistant monosymptomatic NE.12
This case revealed two main points. The first was that suvorexant had a therapeutic effect on a patient with intractable NE by reducing the frequency of NE. Second, the reduction in the frequency of NE may have been due to suvorexant-induced alterations in sleep architecture in the patient, specifically the conversion of deep sleep to lighter sleep.
The author used an approach developed to alter sleep architecture as a treatment for NE in a patient who had failed to respond to all existing treatments. Administration of suvorexant to a patient with uninterrupted NE since birth reduced the frequency of NE by approximately one-third. During the course of treatment, the medication was interrupted two times to confirm the effect of the drug. Each time, the frequency of NE increased until it reached the baseline level, indicating that suvorexant was effective in treating intractable NE.
Suvorexant, an orexin receptor antagonist, is a new drug with a unique clinical profile for the treatment of insomnia. Many currently used insomnia drugs do not have a physiological sleep induction mechanism. They induce sleep by enhancing the action of GABA, an inhibitory neurotransmitter in the brain, thus causing inhibition of the central nervous system.13
In contrast, suvorexant induces sleep through the action of orexin peptides that bind to orexin excitatory receptors in the brain, which are involved in the physiological arousal-inducing mechanism of arousal control. As a result, the administration of suvorexant to insomnia patients does not alter sleep architecture. Indeed, one study found no suvorexant-related differences in sleep architecture between a placebo group and a treatment group.14
Suvorexant increases both N2 and REM sleep.9 This could induce lighter sleep compared with other insomnia medications. To investigate the effects of suvorexant on sleep, sleep polysomnography was performed before and during the administration of medication. In the present patient, suvorexant altered sleep architecture. In terms of overall sleep structure, sleep polysomnography showed an increase in REM sleep, a decrease in non-REM sleep, a decrease in N3 and a corresponding increase in N2 during suvorexant compared with the pretreatment state. Suvorexant administration may have increased REM sleep and decreased N3, which may have resulted in lighter sleep. The effects of suvorexant on sleep architecture were distinct from those of BZDs and non-BZDs when used for insomnia.9 These results suggest that non-REM sleep, especially N3, plays an important role in intractable NE caused by sleep disorders. N2 and REM sleep appear to be important factors in reducing the frequency of NE.
Sleep polysomnography did not have any reported negative effects on the present patient. However, sleep polysomnography assessments should be limited to nonphysiological sleep, such as disturbed or lighter sleep, because polysomnography requires equipment to be attached to the body and the patient to be hospitalised.
The mechanisms by which suvorexant reduced the frequency of NE appear to relate to a decrease in sleep depth, which could facilitate perception of the urge to urinate during sleep, consciously enable inhibition of urination and lower the arousal threshold, which could enable a patient to wake up more easily when they feel the urge to urinate.
Although NE was not completely resolved in the present case, suvorexant substantially reduced the frequency of NE. These data strongly suggest that sleep architecture is implicated in NE. In future, this novel treatment could be applied to patients with intractable NE (especially NE caused by excessive sleep depth), those with NE who are currently receiving other treatments and patients with NE caused by fatigue. This case provides an important clue regarding the cause of NE and will hopefully support the design of future randomised trials.
Learning points
In a 12-year-old boy with severe intractable nocturnal enuresis (NE), suvorexant successfully reduced the frequency of NE by altering the sleep architecture.
Suvorexant may have worked by decreasing sleep depth, thus inhibiting urination and/or facilitating waking.
This treatment represents a novel and effective therapy with potential for treating patients with intractable NE.
Acknowledgments
I thank Dr K Ichiki of Kirigaoka Tsuda Hospital for his comments regarding sleep polysomnography and Sydney Koke, MFA, from Edanz Group (https://en-author-services.edanz.com/ac) for editing a draft of this manuscript.
Footnotes
Contributors TM did all of the planning, treatment practice, data collection, data analysis and interpretation and wrote the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Parental/guardian consent obtained.
Provenance and peer review Not commissioned; externally peer reviewed.