Article Text

Abstract
Giant cell arteritis can result in a wide range of symptoms due to the extensive distribution of the external carotid artery. Face and neck swelling and trismus are under-recognised features of giant cell arteritis and can present as the initial symptom prior to the development of classical temporal tenderness and jaw claudication. The lack of awareness of the less common symptoms may result in a late diagnosis of giant cell arteritis, leading to irreversible vision loss. In this paper, we present a case of neck swelling and airway narrowing as the initial manifestation of giant cell arteritis.
- ear
- nose and throat/otolaryngology
- vasculitis
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Giant cell arteritis is a vasculitis that affects large-sized and medium-sized vessels, including the aorta and branches of the external carotid arteries. Histologically, it is characterised by a granulomatous process with infiltration of multinucleated cells, causing elastic laminae destruction and adventitial fibrosis. The inflammatory process is reflected in blood tests as a raised erythrocyte sedimentation rate and C reactive protein. Diagnosis of giant cell arteritis is based on the American College of Rheumatology’s 1990 guideline, with the presence of three or more criteria out of five.1
Giant cell arteritis is common in the elderly population, with an estimated incidence rate of 15–30 cases per 100 000 individuals.1 Due to the numerous structures supplied by the aorta and the external carotid arteries, giant cell arteritis can produce a broad range of symptoms. The most common symptoms of giant cell arteritis include fatigue, fever, headache, mastication pain and visual changes.
Facial and neck swelling is a subtle change that may feature early and insidiously in giant cell arteritis, although it is seldom reported.2 Other otolaryngologic symptoms including cough, trismus, sore throat, voice changes, dysphagia, hearing loss and tongue claudication.2 3 Aortic involvement can produce thoracic pain, limb swelling and thoracic aortic aneurysm and dissection.
The lack of awareness of the less common symptoms may result in a late diagnosis of giant cell arteritis, leading to irreversible vision loss.
Case presentation
An 87-year-old woman presented repeatedly to the Launceston General Hospital with a history of neck swelling (figure 1). The acute onset of swelling started at the left angle of her jaw and spread inferoanteriorly to her neck. This was associated with trismus-like sensation and dyspnoea. She denied any recent respiratory illness or dysphagia.

Initial presentation with face and neck swelling (A: frontal, B: lateral).
The patient’s medical history included hypertension treated with irbesartan/hydrochlorothiazide, hypercholesterolemia on atorvastatin and osteoporosis on denosumab. In addition, she had been taking aspirin for primary prevention of ischaemic heart disease. There were no medication changes in the preceding 3 years.
During the initial presentation, the patient had a low-grade temperature of 37.8°C and remained haemodynamically stable with a heart rate of 100 bpm, blood pressure of 170/80 mm Hg and an oxygen saturation of 98% on room air. There was no change in voice, stridor, palpable neck nodules or collection on physical examination. The patient was tender over her temporomandibular joints bilaterally and had normal mouth opening to three finger breadths despite sensation of trismus.
Blood investigation revealed normocytic anaemia (haemoglobin of 88 g/L and mean cell volume (MCV) of 89 fL), an elevated white cell count of 17.5×109/L (14.2×109/L neutrophils, 1.4×109/L lymphocyte) and a platelet count of 371×109/L. C reactive protein was elevated at 115 mg/L with a normal antinuclear antibody titre. Thyroid, renal and liver function tests were unremarkable. Contrast-enhanced CT of the neck did not reveal any structural abnormality of the oral cavity, tongue, larynx, thyroid, carotids or lymph nodes other than mild subcutaneous oedema.
The patient was managed as potentially having Ludwig’s angina by the local ear, nose and throat team and was commenced on intravenous piperacillin/tazobactam (Tazocin). A throat swab was obtained, which did not isolate any beta-haemolytic Streptococcus sp. The patient completed 3 days of intravenous antibiotic treatment and was discharged with an oral course of amoxicillin/clavulanic acid (Augmentin Duo forte).
However, she represented 2 days later with worsening of her neck swelling with a new bifrontal headache. Antibiotic was switched to oral ciprofloxacin and clindamycin due to concern of potential betalactam induced angio-oedema.
The patient was reviewed by her general practitioner (GP) 2 days post second discharge and was noted to have worsening erythema over her neck with a fever of 38.4°C. She was transferred back to the Launceston General Hospital (LGH) for further investigations. Clinical examination now revealed trismus, with mouth opening limited to two finger breadths.
Investigations
Blood assays from the third presentation were similar to the first and second presentation (haemoglobin 72 g/L, white cell count 19×109/L, neutrophils 13.3×109/L, platelet 395×109/L and C reactive protein 152 mg/L). Thyroid function tests were deranged with a thyroid-stimulating hormone of 0.14 mU/L and free T4 of 21 pmol/L. Repeated CT scan demonstrated marked inflammation of the lower pharynx and larynx, with swelling of the epiglottis. Severe left-sided wall thickening effaced the left parapharyngeal space, with mild stranding within the peripharyngeal space. Salivary glands were normal and no collections were identified. Severe oedema of the airway resulted in a 14 mm segment of narrowing with a luminal diameter of 2–3 mm (figure 2).

CT showing airway narrowing in (A) sagittal and (B) coronal views.
Twenty milligram of intravenous dexamethasone was administered on receiving the CT findings and an urgent ear, nose and throat review was organised. The flexible nasoendoscopy performed was unremarkable, with normal base of tongue, valleculae, epiglottis and mobile vocal cords. There were no signs of pharyngitis or laryngitis.
Differential diagnosis
Due to the discordance of the CT and direct nasoendoscopy findings, the patient came in under the care of the General Medicine team for further investigations. A wide range of differential diagnoses were considered including atypical infections, drug-induced angio-oedema, hereditary angioedema, autoimmune diseases, haematological malignancy and osteonecrosis of the jaw.
Respiratory multiplex PCR, parvovirus and HIV screen were performed to rule out atypical infections. Aspirin and irbesartan were ceased to rule out drug causes, while a C1 esterase inhibitor and complement levels were organised to investigate hereditary angioedema. Autoimmune screen including antinuclear antibodies, antineutrophil cytoplasmic antibody, extractable nuclear antibody, double-stranded DNA antibodies and erythrocyte sedimentation rate were done, while an orthopantomogram was undertaken and ruled out ONJ (osteonecrosis of the jaw) and local dental infection.
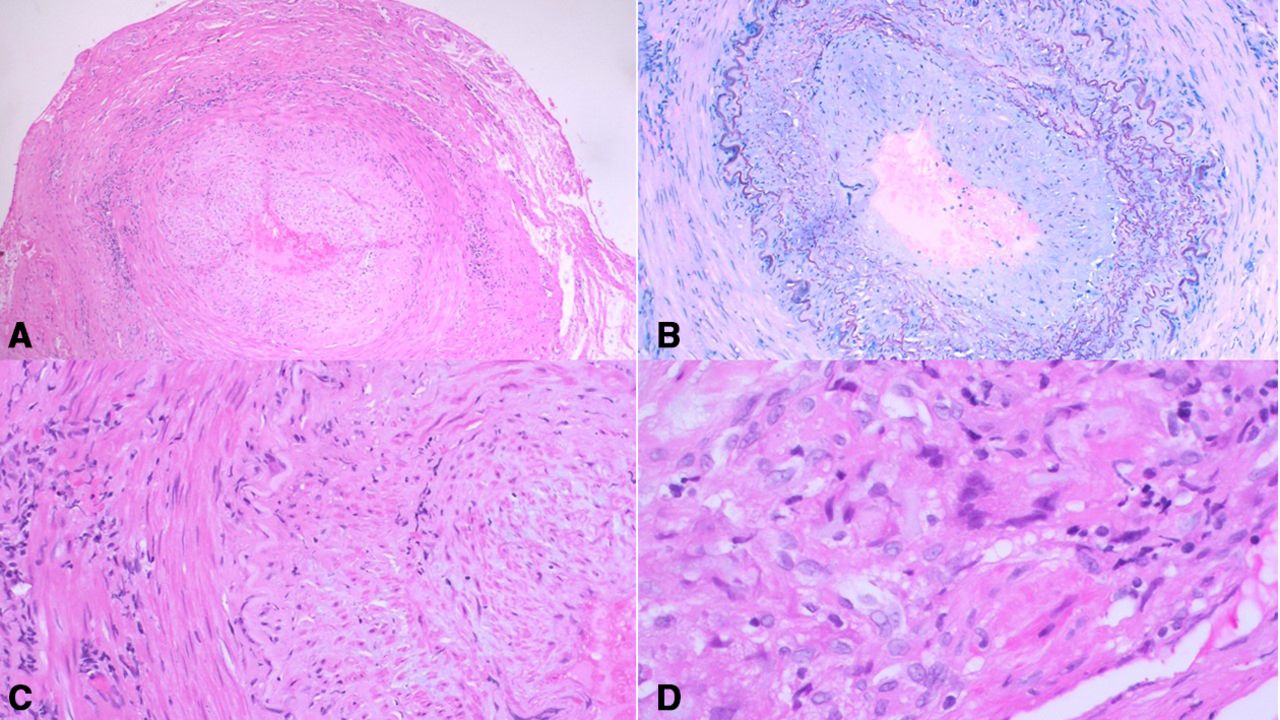
On subsequent review, a more detailed headache history was obtained from the patient. The headache was more severe over the left forehead and was associated with trismus like sensation. Of note, the patient denies any jaw claudication. On examination, the left temporal and frontal regions were tender to palpate, with a palpable vessel noted over the left forehead. The erythrocyte sedimentation rate returned at 121 mm/hour, which raised the suspicion of giant cell arteritis. A left temporal artery biopsy was performed and showed classical findings of giant cell arteritis with fragmentation of elastic lamina, fibrosis of the adventitia and the presence of multinucleated giant cells (figure 3).

Temporal artery histology from patient (A): (H&E 5×) thick-walled artery with an associated inflammatory infiltrate. (B): (Orecin Giemsa 10×) elastin stain highlights fragmentation and reduplication of the elastic lamina. (C): (H&E 20×) narked intimal thickening, smooth muscle disorganisation and adventitial fibrosis. (D): (H&E 40×) lympho-histocystic infiltrate with occasional; multinucleated cells.
TREATMENT
As the patient did not have any ocular involvement at diagnosis, she was started on 50 mg of oral prednisolone per day (1 mg/kg). Adjunctive glucocorticoid-sparing agents such as tocilizumab and methotrexate were considered but due to the dramatic presentation of a threatened airway, a clinical decision was made to streamline treatment with single-agent prednisolone.
Adjunctive methotrexate when used at low doses of 10–15 mg per week has been shown to lower relapse rate, though its glucocorticoid-sparing properties were not evident.4 Tocilizumab, an IL6 receptor antagonist, has demonstrated promising results in reducing glucocorticoid exposure and giant cell arteritis relapse rate, though its role in induction therapy is still yet to be defined.5
Outcome and follow-up
The patient responded to the prednisolone course and had resolution of her facial and neck swelling within 3 days (figure 4). She was discharged home with complete resolution of her symptoms. The high-dose prednisolone was maintained for 4 weeks with a tapering plan of 10 mg reduction every 2 weeks till 20 mg per day. Ongoing weaning will be decided based on clinical symptoms and inflammatory markers at follow-up. At the 6-month phone review, patient remains symptom free on 10 mg prednisolone per day.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Resolution of neck swelling post prednisolone treatment (A): frontal, (B): lateral.
Discussion
Face and neck swelling is a non-specific sign, which has a lengthy list of differential diagnoses. Temporal fossa swelling is well recognised in giant cell arteritis however face and neck swelling is less common, occurring in 6.5% of cases.2 The swelling follows a waning and waxing pattern and may be due to spasm and collateralisation of the facial artery.2 6 7 The raised inflammatory markers can cause physicians to treat the initial presentation as an infection and to attribute the resolution of swelling to antibiotic response, as illustrated in our case.
Trismus (reduced jaw opening) has a prevalence of 6.8% in giant cell arteritis but is seldom reported due to its overlap with jaw claudication.8 Our case demonstrates that trismus can occur in isolation from jaw claudication. The mechanism for trismus in giant cell arteritis is uncertain but thought to be due to restricted blood flow to the masseter muscles via distal branches of the external carotid arteries.9 Interestingly, the patient developed subclinical hyperthyroidism during her admission, though it is uncertain if this is related to giant cell arteritis affecting the superior thyroid or a sick euthyroid state. Thyroid dysfunction has been described in giant cell arteritis, though no clear correlation was established due to the overlapping patient epidemiology of giant cell arteritis and thyroid diseases.10 11
The third presentation with airway narrowing stipulated a revisit of the patient’s diagnosis and presented as one of the first cases of CT-documented airway narrowing secondary to giant cell arteritis. Inflammation of the external carotid artery, where the superior laryngeal artery originates from, likely caused local ischaemia and oedema of the superior larynx. Fortunately, for the patient, giant cell arteritis was recognised early in her illness, with complete resolution of symptoms once corticosteroid treatment was commenced.
Patient’s perspective
Patient’s perspective (written with assistance from her daughter)
The whole situation is like going on an adventure, but it was not a good adventure. Not being diagnosed for 2 weeks with a swollen jaw was horrible. For my third trip to the hospital, I was not able to open my jaw and can only eat baby food. Having a doctor who found a diagnosis for me was a relief. When they started treatment, my frightening condition eased quickly.
Learning points
Giant cell arteritis can result in a wide range of symptoms due to the extensive distribution of the external carotid artery.
Face and neck swelling and trismus are under-recognised feature of giant cell arteritis and can be transient prior to developing classic giant cell arteritis symptoms.
Trismus can occur in isolation from jaw claudication in giant cell arteritis.
We recommend that any patient above the age of 50, who presents with face and neck swelling or trismus, to have giant cell arteritis considered as a differiential diagnosis.
Footnotes
Contributors This case was managed by CS as the Consultant, with ZSL as the Medical Registrar. ZSL wrote up the case with supervision, some direction and editing by CS.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.