Article Text

Abstract
Traumatic intrusion is considered one of the most severe luxation injuries to the permanent dentition. There are limited studies based on minimal evidence supporting suggested management protocols, owing to the rare occurrence of intrusion. The following case report details the multidisciplinary management and 18-month follow-up, in line with current UK guidelines, of a 23-year old adult male who sustained severe intrusion injuries to both permanent maxillary central incisor teeth. Timely, accurate diagnosis and subsequent appropriate management correlates with improved outcomes for traumatic injuries and it is therefore imperative those involved with the acute and long-term management of dentoalveolar trauma are aware of current guidelines.
- dentistry and oral medicine
- accidents
- injuries
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Five per cent of all injuries requiring acute treatment are related to dental trauma.1 2 Intrusion injuries have a reported incidence of 0.5%–2% of all dental trauma with a predilection towards males.1 By definition, intrusion presents as apical displacement of a tooth into alveolar bone. The resulting damage to periodontal ligament, root cementum, neurovascular bundle and surrounding alveolar bone can severely compromise the long-term prognosis of the affected permanent dentition.3 Of these cases, 97.2%occur in the anterior maxilla (upper canine-canine teeth).1
Given the relatively rare presentation of dental intrusion injuries, management protocols are based on limited evidence and several forms of guidance exist.4–6 Short-term management of intrusion injuries may include surgical or orthodontic repositioning of traumatised teeth and provision of a flexible trauma splint. Improved outcomes of treatment have correlated with timely and appropriate management.7 In the permanent dentition, pulp necrosis may occur in 88%–98% of intruded teeth with complete root development and subsequent endodontic treatment is necessary.5 8 Even with optimal immediate and long-term management, root resorption can occur in 51%–73% of cases, leaving affected teeth with a guarded long-term prognosis.8–10 This may ultimately result in early loss of teeth.
Case presentation
A fit and well 23-year old man presented to a dental hospital after sustaining dental trauma falling onto the back support of a dining room chair. The patient presented to an accident and emergency (A+E) department where he was assessed by oral and maxillofacial (OMFS) clinicians. An orthopantomogram (OPG) was requested to assess facial fractures was ordered by our OMFS colleagues at the time of presentation to the accident and emergency department. He was discharged without treatment and advised to seek further management by his general dental practitioner. He presented to a dental hospital 36 hours following injury. His medical history was unremarkable.
Investigations
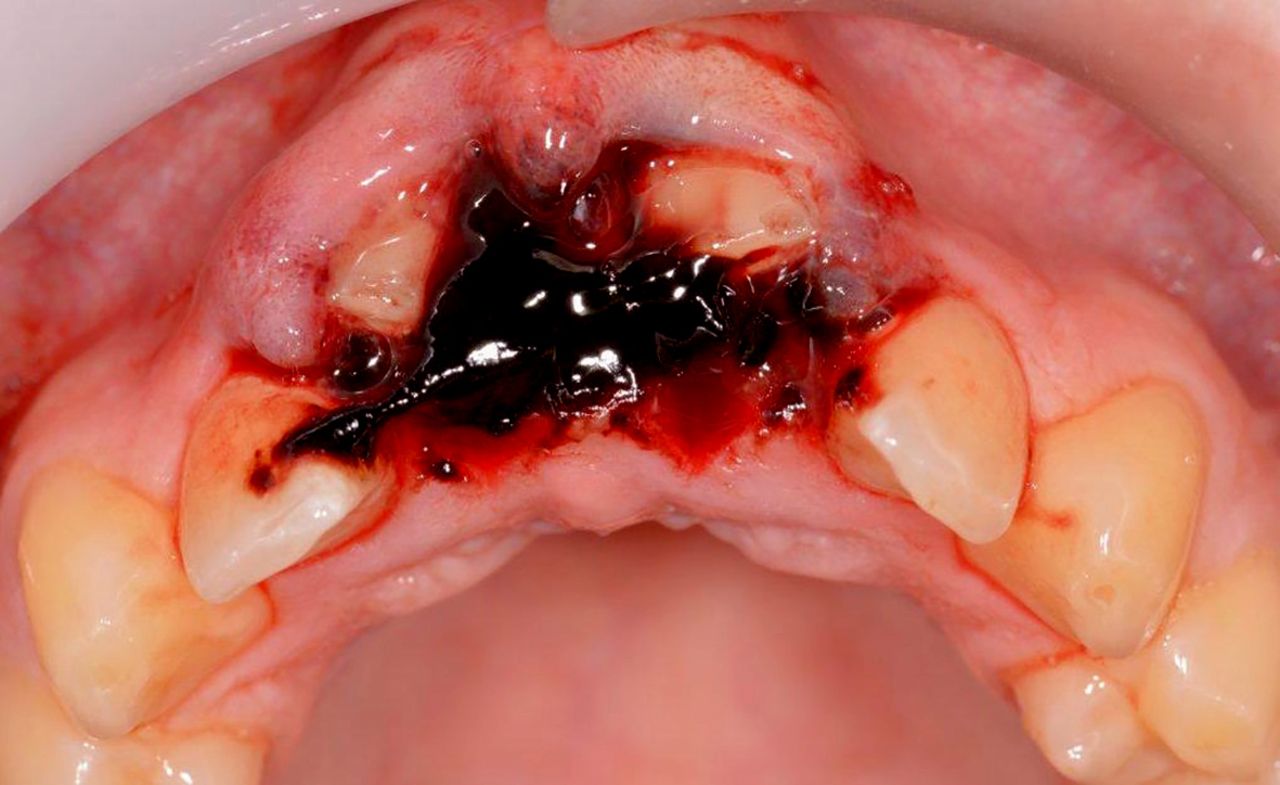
On assessment 36 hours following trauma, relevant clinical findings included abrasions to the upper lip, haematoma around the gingival sulcus in the maxillary central incisor region and the crowns of both maxillary central incisor teeth (11 and 21) appeared apically displaced into the maxillary alveolus with incisal edges partially visible (figure 1). The apices of the maxillary central incisors could be palpated during the extra-oral examination at the nasal sill. Initial pulp sensibility, percussion and mobility of adjacent teeth (maxillary lateral incisors, canines and mandibular incisors) were unremarkable, while the traumatised maxillary central incisors gave negative thermal responses and positive tenderness to percussion. Given the extent of the intrusion and the completed root development, it was accepted that pulp necrosis would occur in both maxillary central incisors.5 11

Initial presentation 36 hours following injury. Incisal edge of maxillary central incisors partially visible.
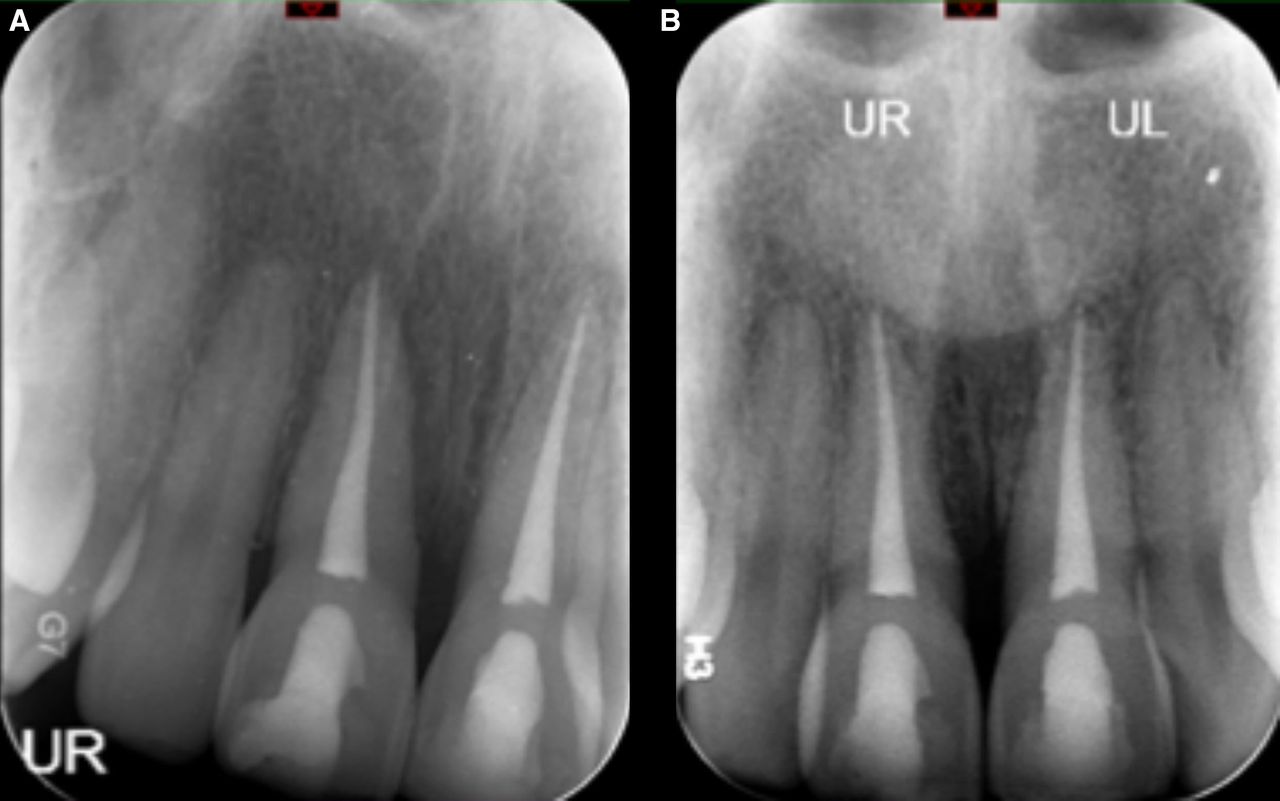
Radiographic examination with intra-oral and extra-oral films—periapical, maxillary occlusal and OPG views, corroborated the clinical findings that teeth 11 and 21 were intruded by 9 mm (figures 2–4).

Standard maxillary occlusal radiograph identifying apical displacement of the maxillary central incisors (36 hours following injury).

Periapical radiographs suggesting apical displacement of the maxillary central incisors (36 hours following injury).

An orthopantomogram confirming severe apical displacement of the maxillary central incisors and ruled out facial fractures taken within the accident and emergency department following trauma (radiolucency suggestive of caries to be managed by the general dental practitioner).
Treatment
Immediate management, under local anaesthetic delivered using buccal and palatal infiltrations, included debridement of soft tissue abrasions, surgical repositioning of both maxillary central incisor teeth with extraction forceps and provision of a titanium trauma splint bonded to all maxillary incisors (figure 5). No gross contamination of the wound was evident and thus antibiotic prescription was not administered. Following repositioning, no displacement of soft tissue was evident, the affected papillae were well approximated and suturing was not performed in this case. Suturing may benefit in case with detached papillae. Endodontic treatment of the teeth 11 and 21 was initiated 2 weeks following trauma. An interappointment non-setting calcium hydroxide dressing was provided to prevent the development of inflammatory (infection-related) external resorption.11 Seven weeks following trauma, the splint was removed and orthograde endodontic treatment was completed using gutta percha via the warm vertical condensation obturation technique (figure 6). While there was no evidence of complete alveolar fracture through both the palatal and the labial alveolar plates with a mobile alveolar segment, the positioning of the apices in relation to the labial bone suggested labial plate fracture, and at initial review, it was decided to extend splinting to a total of 7 weeks.
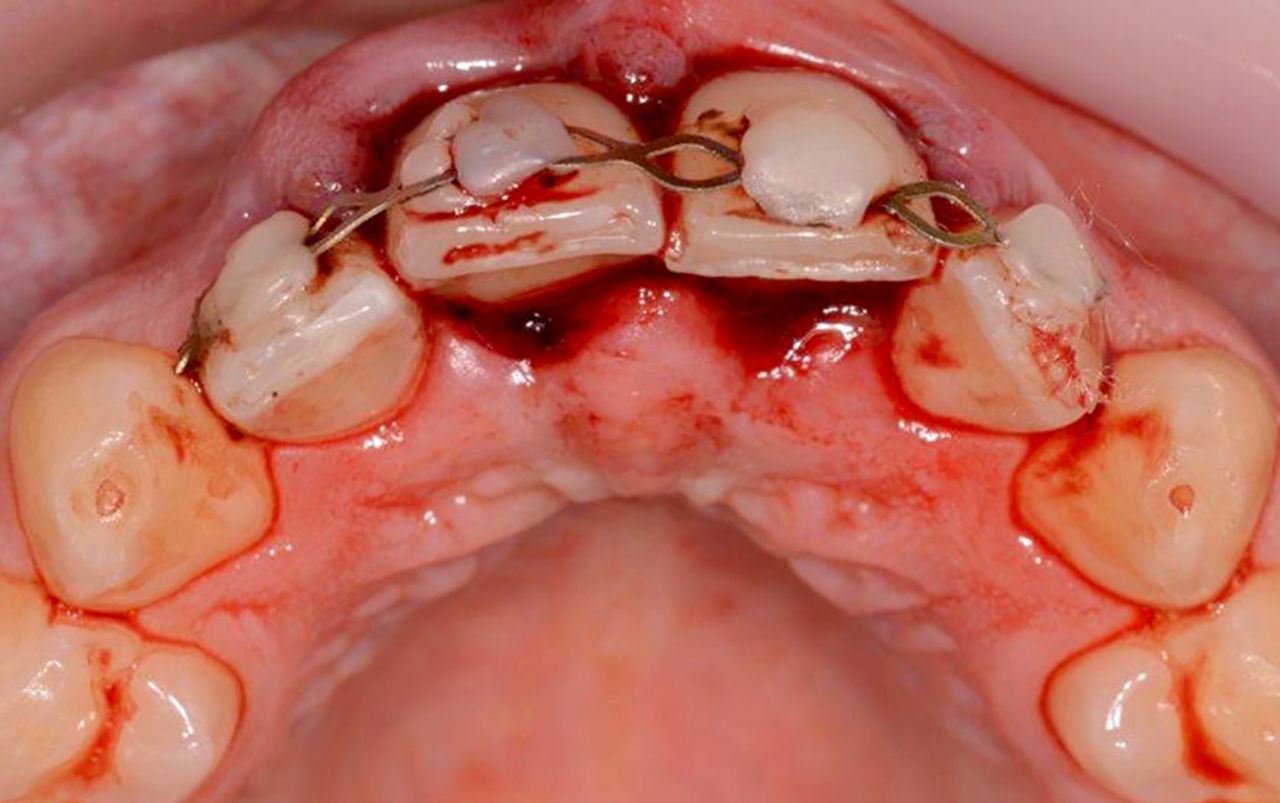
Provision of titanium trauma splint following surgical repositioning of maxillary central incisors (36 hours following injury).

Periapical radiographs showing maxillary central incisors immediately following endodontic treatment (7 weeks following injury).
Outcome and follow-up
Clinical and radiographic review followed published guidance.5 11 Pulp sensibility, percussion and mobility testing of adjacent teeth (maxillary canines and lateral incisors) remained unremarkable. Clinically, a high-pitched metallic sound, suggestive of external replacement root resorption (ERRR), was exhibited on percussion testing of the left maxillary central incisor from 29 weeks post trauma (figure 7). There was minimal radiographic evidence suggestive of replacement resorption (figure 8A,B) over an 18-month review period. In light of the ankylotic sound exhibited on percussion, further annual clinical and radiographic review including cone-beam CT (CBCT) is planned to monitor ERRR progression. The position of both central incisors is acceptable to the patient; the patient had an existing anterior open bite prior to injury. Mild incisal edge discrepancies that persist following repositioning can be managed restoratively with composite edge bonding. Large discrepancies or other malocclusions may require orthodontic intervention.

Eighteen-month postoperative clinical views, evidence of marginal bone loss around maxillary central incisors present interproximally.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Periapical radiographs showing maxillary central incisors at 6-month (left) and 18-month (right) review following endodontic treatment.
Discussion
Epidemiology
Intrusion is a rare form of dental trauma. An epidemiological study involving 216 intruded teeth displayed a prevalence of intrusion in 1.9% of all traumatic dental injuries over a 50-year period in Europe.1 The main aetiological factor appeared to be falling, as in this case, resulting in impacts acting axially along affected teeth. Coincident dental injuries occurred in 66.5% of teeth, predominately involving crown fractures.1 Of these cases, 53.7% involved intrusions of more than one tooth.1
Presentation
Clinical presentations include crown submergence, gingival lacerations, lack of mobility and a metallic sound on percussion of the intruded tooth/teeth. Intrusion may present radiographically as displacement of a root apex (this may present as foreshortening of roots should there be displacement in an anteroposterior direction). Radiographically, the periodontal ligament space around a root apex may appear obliterated. The majority of intrusion injuries are displaced within a range of 1–8 mm.7 10 Accurate and comprehensive diagnosis may be aided by radiographs at several angles such as a combination of occlusal and periapical views of the affected teeth.1 2 Parallax views may also reveal dentoalveolar fractures or signs of further damage to traumatised teeth outside the plane of a single view.4 While readily available in a hospital setting, extra-oral films, such as an OPG, may not show sufficient detail to identify root or alveolar fractures. Therefore, use of adjunctive intra-oral films, such as standard maxillary occlusal and periapical radiographs, is recommended.
Management and complications
Acute management protocols aim to restore intruded teeth to their original position, either via orthodontic or surgical positioning, in the hope of re-establishing a pre-existing relationship between the tooth and bone.12 13 Given the sparsity of evidence comparing the efficacy of different treatment options, there is diverging opinion on a superior management option.4–6 However, recent UK-based guidance, following thorough review of published literature, provides a consensus on accepted management protocols and is summarised in table 1.5 Allowing spontaneous re-eruption, otherwise known as passive repositioning, may be advised in cases of mild intrusion (<3 mm) with mature apices.5 Active repositioning via orthodontic means is advised should no coronal movement occur 2–3 weeks following trauma.5 Moderately displaced (3–6 mm) permanent teeth with mature apices require ‘active repositioning’ either surgically or orthodontically. Surgical repositioning, seen in this case, is justified when managing severely intruded teeth (>6 mm).5 Since the management of this case, international guidance has been published advocating identical management protocols with ranges of ‘moderate’ displacement amended to 3–7 mm.11
Summary of treatment recommendations for intruded teeth based on UK guidance5
Acute management adjuncts may involve splinting and/or antibiotic prescription. The splinting of repositioned teeth using a non-rigid, flexible splint has been strongly recommended in recent guidance.4 5 One sound tooth, either side of the traumatised teeth should be splinted.14 Splinting for a period of 6–8 weeks has been recommend by Andreasen et al.15 However, splinting for 10 days has also been shown to reduce mobility sufficiently enough to allow function.12 There is limited evidence corroborating the administration of systemic antibiotics to aid pulpal or periodontal healing. However, clinical judgement may be exercised in cases with contamination of associated soft tissue injuries.5
Subsequent collateral damage to dentine, cementum, periodontal ligament and alveolar bone may result in significant long-term complications such as pulp necrosis, infection of the root canal system, marginal bone loss, root resorption and subsequent tooth loss.16 17 The prevalence of pulp necrosis in intruded teeth with complete root development is estimated to occur in 88%–98% of cases.5 Early endodontic treatment is advised and should be initiated within 2 weeks of trauma or as soon as the position of the tooth allows.11 Thus, long-term follow-up of teeth is advised in multiple guidance documents.1 4 5 The three-dimensional capability of CBCT is reported to be more sensitive than periapical radiographs in identifying apical changes and is useful when assessing teeth with suspected root resorption.18 19
Pulp necrosis, as a result of apical displacement of the tooth, may occur as the pulp’s main blood supply, via the apical foramen, is severed.20 21 Resorption, which is defined as ‘progressive loss of cementum and dentine through continued osteoclastic activity’, may be initiated and/or maintained following substantial damage to cementum and the periodontal ligament.17 22–24 Injury severity correlates with the extent of resorption.25–27 Younger patients may be at greater risk of rapid resorption.28 Substantial damage may result in complete resorption of the root. In adults, this may take up to 20 years; however, in children, tooth loss as a result of this resorptive process may occur in 3–7 years.26 29 In light of the extremely high risk of pulpal necrosis and resorption in cases with moderate or severe intrusion, prompt onward referral for further specialist dental assessment is required.
Marginal bone loss is a commonly documented sequalae of traumatic intrusion, especially in cases of multiple intrusion injuries.30 31 Marginal bone loss following intrusion injuries appears to occur as a result of the crushing of the surrounding alveolar bone as well as exposure of bone to the oral cavity. As Tarnow et al highlights, the position of crestal bone relative to the contact point greatly influences the position of the papillae.32 This would explain the loss of papillae interproximal to the maxillary central incisors in this case (figure 7). This was an acceptable aesthetic outcome for the patient, which would otherwise require restorative treatment, orthodontics or periodontal surgery to correct.33
Delays in the acute management of intrusion injuries may complicate repositioning and further increase prevalence of pulp necrosis, resorption and compromise aesthetics.7 16 In this case, immediate referral to a specialty dental setting may have further optimised treatment outcome by enabling rapid surgical repositioning and commencement of root canal treatment within the recommended 2-week window following trauma.5 Delaying endodontic treatment longer than this time has been correlated with a higher prevalence of root resorption.34 This may increase the risk of subsequent tooth loss, which is heavily implicated in quality of life.35
Learning points
The occurrence of dental intrusion is rare.
Given the large forces required to illicit such an injury, damages to tooth and surrounding structures can be extensive and may have profound complications that may significantly compromise the long-term prognosis of intruded teeth.
Acute management, in the form of surgical repositioning and the provision of a flexible trauma splint, is simple and should be accessible to those working in acute care settings.
Given the poor prognosis of dental intrusion injuries, immediate onward referral for multidisciplinary specialist input may optimise long-term treatment outcomes.
Awareness of up-to-date guidance on the management of intruded teeth is imperative among clinicians working in acute care settings.
References
Footnotes
Twitter @LongridgeNick
Contributors The following authors were involved in the submitted article: AR-W, NL, SMK. SMK led the initial management (initial assessment and surgical repositioning and provision of trauma splint for patient). NL provided subsequent root canal therapy of both central incisors. SMK and NL were both involved in the follow-up. AR-W was involved in the inquisition, reporting and analysis of data, and drafting of the submitted article.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.