Article Text

Statistics from Altmetric.com
Description
A 43-year-old woman was referred to our thoracic surgery department following multidisciplinary team (MDT) discussion for a concerning 7×5 mm pulmonary nodule in the medial right upper lobe which was discovered incidentally on a CT thorax abdomen pelvis (figure 1) as part of surveillance for her previous cervical cancer. This woman has a history of squamous cell carcinoma of the cervix (stage IIB), which was diagnosed in 2012 and managed with chemoradiotherapy. Unfortunately, she had a number of complications secondary to radiotherapy including a colovesical fistula (2013), defunctioning loop ileostomy formation (2014), vesicovaginal fistula (2014) and recurrent urirnary tract infection (UTIs). In late 2014, she developed a 4 cm cutaneous squamous cell metastasis in her right flank which was surgically excised. Her other medical history includes lupus and hypothyroidism. She is a non-smoker. Following identification of the pulmonary nodule on CT TAP, she underwent PET CT. However, the subcentimetre nodule was too small to resolve with PET and remained indeterminant. No other concerning areas of uptake were identified. The differential diagnosis clinically was metastatic cervical carcinoma or a primary lung neoplasm. She subsequently underwent right video-assisted thoracoscopic surgery upper lobe wedge resection.

CT thorax abdomen pelvis—new 7x5 mm nodule in medial right upper lobe.
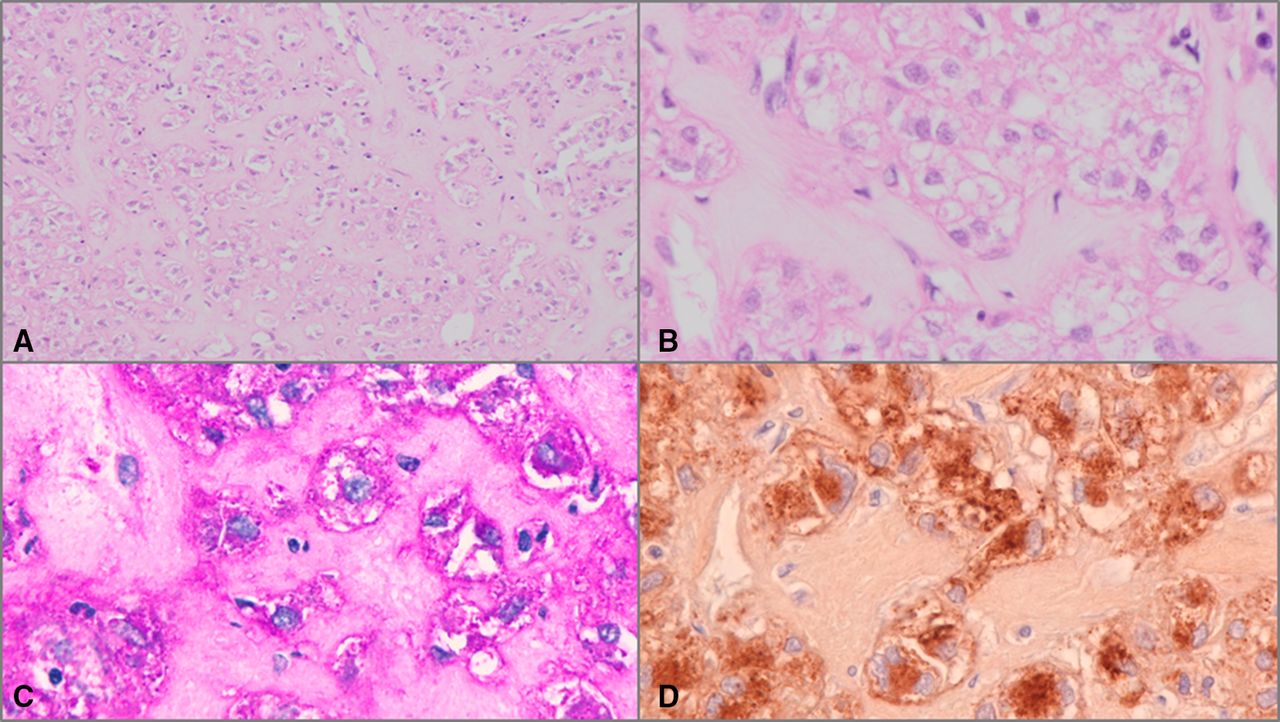
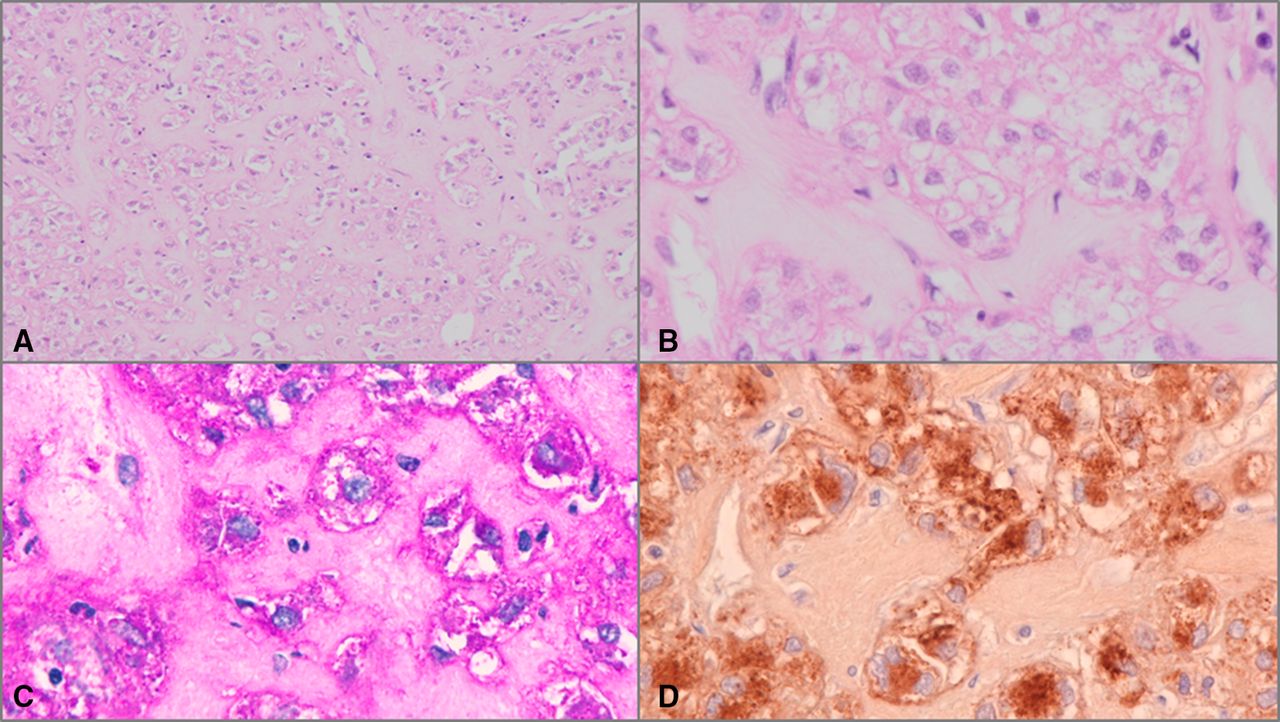
Macroscopic examination of the lung wedge revealed a circumscribed, firm, white nodule, measuring 7 mm in largest dimension, excised by 1 mm to the closest resection margin. Microscopic examination revealed the nodule to be a well-circumscribed tumour composed of nests of bland cells with clear and granular cytoplasm, set in a hyalinised stroma (figure 2). Significant cytological atypia was not seen. Mitoses were not evident. Immunohistochemistry showed that the lesional cells stained positively for HMB45, with focal positivity for melan A. The cytoplasmic granules stained positively with periodic acid–Schiff and negatively with periodic acid–Schiff diastase, confirming the presence of glycogen. Immunohistochemistry for SOX10, S100, desmin, synaptophysin, PAX8, ERG, oestrogen receptor, AE1/3, p63, CK5/6, TTF-1 and napsin A were negative. Features of metastatic squamous cell carcinoma were not seen. Following histopathological analysis (figure 2), the diagnosis of clear cell ‘sugar’ tumour (CCST) of the lung was made that showed no malignant features. As this was a benign pulmonary lesion, this woman’s follow-up will be guided by her primary cervical cancer.
{kind=link}
{kind=link}
(A) nests of bland cells with clear and granular cytoplasm within a hyalinised stroma, H&E stain ×100 magnification, (B) H&E stain x400 magnification, (C) positive cytoplasmic periodic acid–Schiff staining of glycogen within tumour cells, x400 magnification, (D) tumour cells showing positive HMB45 immunohistochemistry, x400 magnification.
CCST has been recently recognised to belong to the perivascular epithelioid cell tumour (PEComa) family of tumours.1 These are rare mesenchymal neoplasms that appear to arise from perivascular epithelioid cells and have morphological, immunophenotypic and ultrastructural similarities. PEComas usually have a combined myogenic and melanocytic immunophenotype. They occur more commonly in women. PEComas include specific entities such as CCST of the lung, angiomyolipoma and pulmonary lymphangioleiomyomatosis, and can occur as PEComas in the viscera, soft tissue and skin. Most PEComas are sporadic, but an association with tuberous sclerosis complex has been shown in angiomyolipoma, lymphangioleiomyomatosis and very rarely CCST.1
CCST is a rare tumour arising in the lung. It was first described by Liebow and Castleman.2 CCST usually arise in the periphery of the lung, are often incidentally detected, and can measure up to 7 cm in size. They are composed of nests of uniform cells that have both clear and granular cytoplasm, well-defined cell borders and lack cytonuclear atypia and mitoses.1 The cytoplasmic granules are composed of glycogen, which stain positively with periodic acid Schiff. Dilated vascular spaces surrounded by walled vessels are prominent. Necrosis and haemorrhage are not seen. Some cells may have a spindled morphology and stain positively with actin. Tumour cells should stain positively with melanocytic markers such as MiTF, Melan A and HMB-45 and negatively with epithelial markers.3 S100 may be positive.
The pathological differential diagnoses include pulmonary metastasis of clear cell renal carcinoma, primary clear cell carcinoma of the lung, paraganglioma, primary intrapulmonary meningothelial neoplasm and malignant melanoma.4
Most clear cell ‘sugar’ tumours of the lung behave in a benign fashion but eight potentially malignant or malignant cases have been reported to date in the literature.4 Zhao et al proposed criteria for malignancy as follows:
Primary diagnostic criteria: prominent coagulative tumour necrosis, infiltration of adjacent pleura or viscera, distant metastasis of homology, pathological mitotic figure ≥1/50HP (high power).
Secondary diagnostic criteria: tumour size ≥3 cm, spotty necrosis, high mitotic index ≥5%, multinucleated tumour giant cells≥5/50HP, marked hypercellularity, nuclear atypia and pleomorphism, numerous intranuclear pseudoinclusions.4
The criteria for the diagnosis of malignant lung PEComa that they recommend are that the tumour meets 1–2 major diagnostic criteria and/or one more secondary diagnostic criterion. If the tumour satisfies only two or more secondary diagnostic criteria, they suggest the diagnosis of lung PEComa with malignant potential.4
Using these diagnostic criteria, this case of CCST would be classified as benign. However, due to the rarity of these lesions, it is difficult to be certain at present of their clinical behaviour.5
Learning points
Clear cell ‘sugar’ tumour of the lung is a rare benign lung tumour usually arising in the periphery of the lung and often detected incidentally.
The tumour cells should stain positively with periodic acid–Schiff due to cytoplasmic glycogen granules and also stain positively with HMB45/Melan A demonstrating the melanocytic immunophenotype.
Criteria for malignancy seen in rare cases include tumour size ≥3 cm spotty or coagulative tumour necrosis, high mitotic index ≥5% with atypical mitoses, multinucleated tumour giant cells≥5/50HP, marked hypercellularity, nuclear atypia and pleomorphism, numerous intranuclear pseudoinclusions infiltration of adjacent pleura or viscera and distant metastasis.
Ethics statements
Patient consent for publication
Acknowledgments
Thank you to the patient for kindly allowing us to submit the case.
Footnotes
Twitter @lukeob13
Contributors LMO - manuscript preparation & junior doctor caring for patient. RT - manuscript preparation & registrar reading histopathology slides. MT - manuscript editing & consultant caring for patient. AF - manuscript preparation & consultant reading histopathology slides.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.