Article Text

Statistics from Altmetric.com
Description
A 54-year-old woman presented with 7 days of monocular left blurred vision and floaters with best-corrected visual acuity (BCVA) of 6/15–2. She had no significant medical history. Headache was investigated elsewhere 4 weeks previously with negative temporal artery biopsy; however, temporal arteritis was treated empirically with oral steroids.
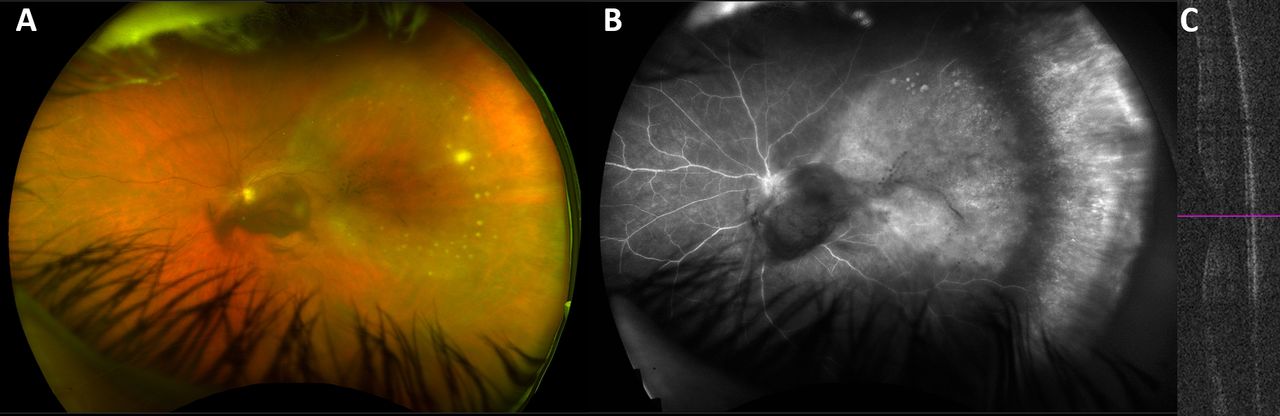
Examination showed 1+ anterior chamber cells, intraocular pressure of 14 mm Hg, no cataract but dense central vitritis. A wedge-shaped area of temporal retina was outlined by white dot intraretinal infiltrates (figure 1A). Fundus fluorescein angiography (FFA, Optos plc, Scotland) showed nasal retinal vasculitis and diffuse temporal hyperfluorescence with obscured retinal vasculature (figure 1B) corresponding to the wedge-shaped area. Macular optical coherence tomography (OCT, Cirrus 5000, Carl Zeiss Meditec, USA) was normal (figure 1C). The working diagnosis was panuveitis with diffuse temporal retinitis and retinal vasculitis.
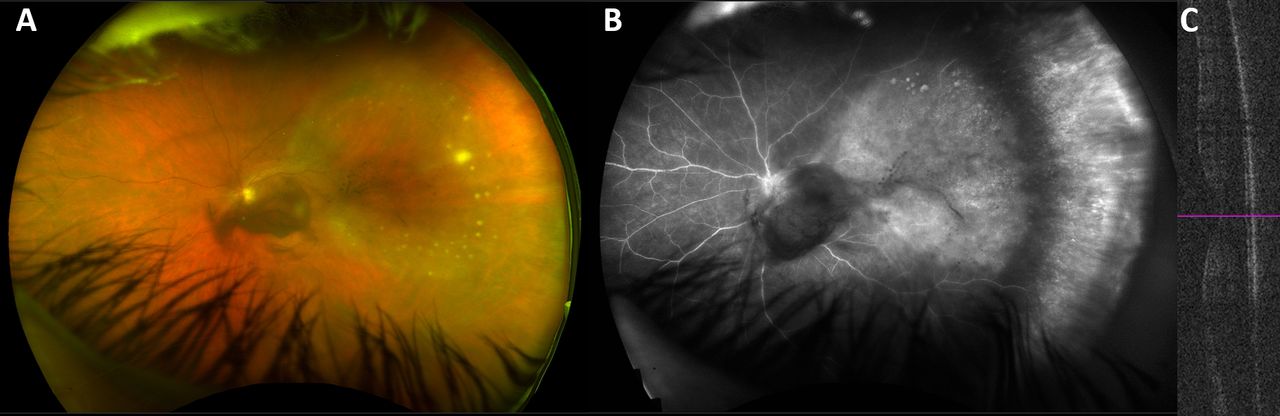
(A) Widefield colour photograph of the left fundus showing two clusters of central vitritis with wedge-shaped temporal area of abnormality surrounded by intraretinal white dots. (B) Late phase wide-field FFA of the left fundus showing nasal retinal vasculitis with a well-circumscribed temporal wedge-shaped area of hyperfluorescence; note, the intraretinal white dots are not uniformly apparent on FFA. (C) OCT image showing normal retinal structure with obscuration by vitritis artefact. FFA, fundus fluorescein angiography; OCT, optical coherence tomography.
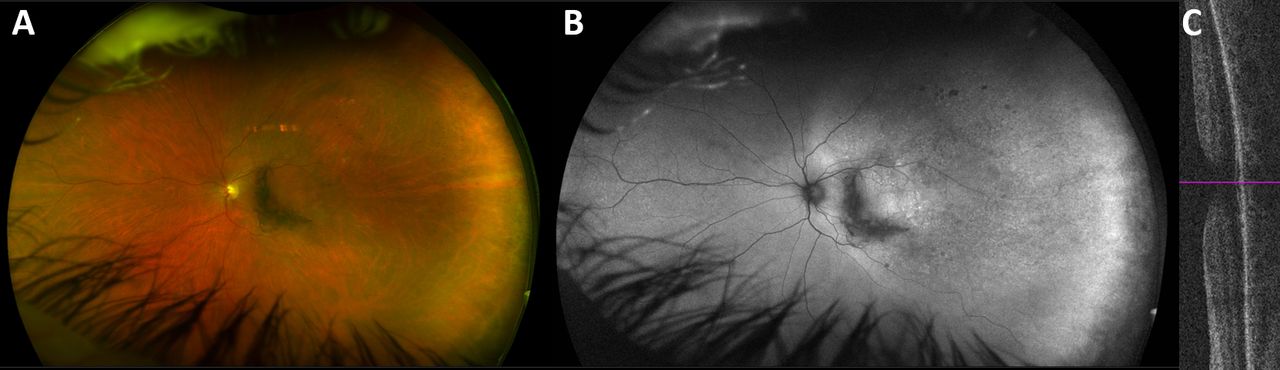
Serum and aqueous humour were negative for tuberculosis, Borrelia and Toxoplasma. Treponema pallidum rapid plasma reagin (RPR) serology was elevated at 1:256 prompting 14-day treatment with intravenous benzylpenicillin. Further investigations showed negative HIV serology, normal cerebrospinal fluid (CSF) analysis and cerebral vasculitis on neuroimaging. BCVA improved to 6/7.5 with reduction of vitritis and resolution of intraretinal infiltrates (figure 2A) leaving a large area of mottled hyperautofluorescence (figure 2B). OCT remained normal (figure 2C).

{kind=link}
{kind=link}
(A) Widefield fundus photograph of the left fundus 4 weeks after systemic antimicrobial treatment with dramatic improvement in vitritis, resolution of ‘active’ intraretinal white dots and development of fine round intraretinal pigmentation, indicative of resolved inflammation. (B) Widefield autofluorescence image showing a large temporal wedge of mottled hyperautofluorescence which is larger than the original clinically apparent extent of retinitis. (C) Optical coherence tomography showing preserved foveal outer retinal architecture, absence of macular oedema and clearing vitreous artefact.
Syphilis is a sexually transmitted infection with an estimated prevalence of 0.5% in adults <50 years.1 It accounts for 10% of infectious uveitis.2 Syphilitic uveitis (SU) typically denotes secondary syphilis; however, ocular involvement may occur in any stage.1 Meningovascular syphilis manifests in 3% of untreated syphilis infections comprising cerebral vasculitis with headache, motor/behavioural change or even stroke.3 ‘The great imitator’, ocular syphilis requires a high index of suspicion with myriad presentations including panuveitis (75%), anterior uveitis (66%), papillitis (88%) and retinitis/vasculitis (72%).1 4 5 SU is bilateral in >60%, typically with HIV coinfection (70%); thus, HIV testing in primary or secondary syphilis is prudent.5–7 Standard syphilis tests include screening by enzyme and chemiluminescent immunoassays, to detect antitreponemal antibodies, confirmed by the RPR test.5 Neurosyphilis manifests in 10% of untreated cases and SU should be managed as neurosyphilis (ie, CSF analysis, neuroimaging and therapy5). FFA and OCT are useful adjuncts assessing chorioretinal involvement (eg, early phase FFA ‘Leopard spotting’ or hypofluorescent spots overlying acute syphilitic posterior placoid chorioretinal lesions6).
Parenteral penicillin (eg, intravenous benzylpenicillin or intramuscular procaine penicillin) is recommended for 10–14 days7 with cephalosporin/macrolide alternatives in penicillin-allergic individuals. Treatment success has been reported in up to 90% of cases.7 The Jarisch-Herxheimer reaction (ie, endotoxin-mediated systemic inflammatory response) occurs in up to 75% of patients after antimicrobial treatment of spirochaetal infections (eg, Treponema, Borrelia); thus, systemic steroids are appropriate to ameliorate these reactions.8
Ocular syphilis is challenging due to its array of manifestations1 2 4 5 with early diagnosis crucial as infection >28 days is associated with poor visual outcomes.6 This case is atypical as eye involvement was unilateral, cerebral vasculitis was seen, HIV test was negative and outcome was good despite delayed presentation.
Learning points
‘The great imitator:’ a high index of clinical suspicion for syphilitic uveitis is good practice, particularly in high-risk cohorts (eg, HIV coinfection).
Multimodal retinal imaging is useful in syphilitic uveitis to clarify the extent and severity of posterior segment inflammation as well as to monitor treatment response.
Infective causes of uveitis (eg, T. pallidum, M. tuberculosis, B. burgdorferi) must be excluded prior to systemic immunosuppressive therapy as inappropriate immunosuppression may cause ocular or systemic deterioration.
Ethics statements
Patient consent for publication
Acknowledgments
The authors would like to thank the Photographic Department of the Royal Victoria Eye and Ear Hospital, Dublin, Ireland.
Footnotes
Twitter @OcularOirg
Contributors DH and KGS: manuscript construction and revision. KAJS and CCM: diagnosis/clinical care, manuscript construction and revision.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Author note Twitter: Deirdre A Harford @DeirdreHarford; Kirk AJ Stephenson @KarkStaphonsen;
Conor C Murphy @OcularOirg