Article Text

Statistics from Altmetric.com
Description
It is generally presumed that large neck masses resulting in airway obstruction are associated with a primary neoplastic problem in the upper aero-digestive tract mucosa, usually a carcinoma. Metastasis into the neck from regions below the diaphragm, such as the prostate, though not unknown, is very rare. We present a case of airway obstruction due to metastatic prostate carcinoma within the thyroid cartilage.
A 66-year-old man with a background of metastatic prostate carcinoma and enlarging left neck lump (level 2–3) for 8 months presented to us with airway compromise and required an urgent tracheostomy.
A recent MRI demonstrated a left-sided mass arising from the thyroid cartilage, crossing the midline and encroaching towards the larynx with considerable airway compromise. There was complete destruction of the left lobe and lower pole of the right lobe of the thyroid gland with enlarged cervical lymph nodes at level II and III on the left (figures 1 and 2).

MRI of the neck (T1-weighted)—coronal slice demonstrating a large, lobulated, heterogeneously enhancing, left-sided, 7×5.1×5.3 cm neck mass arising from the thyroid cartilage and crossed the midline. Arrow indicates narrowest point of airway. A, airway; L, left; M, mass; R, right; T, thyroid cartilage; *cricoid cartilage.

{kind=link}
{kind=link}
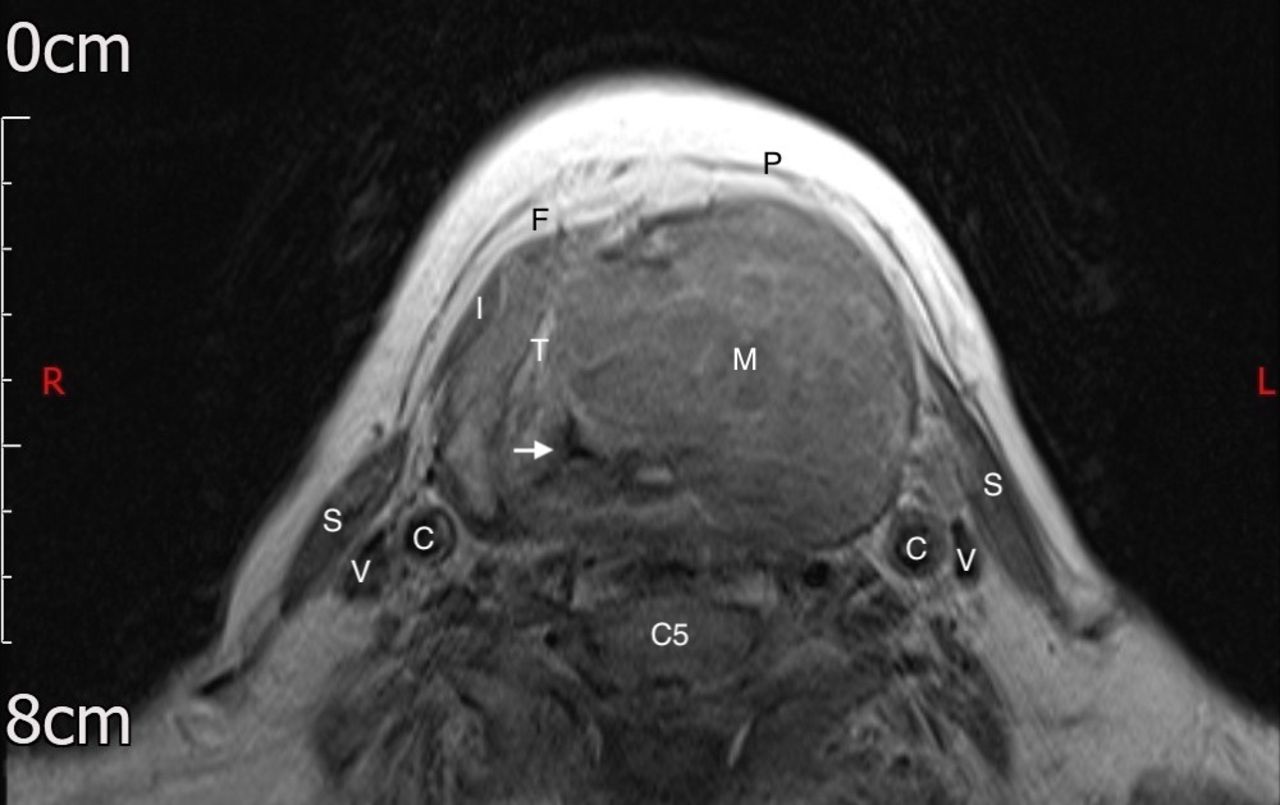
MRI of the neck (T1-weighted)—axial slice at level of thyroid cartilage and C5 cervical vertebra demonstrating large, left-sided neck mass compressing the airway. Arrow indicates narrowest point of airway. C, common carotid arteries; C5, vertebral body of fifth cervical vertebra; F, investing layer of deep cervical fascia; I, infrahyoid (STRAP) muscles; L, left; M, mass; P, platysma muscle; R, right; S, sternocleidomastoid muscles; T, thyroid cartilage; V, internal jugular veins.
Under strict vigilance in the operating theatre and precautionary plans, the patient was successfully intubated before tracheostomy and biopsy of the mass through the tracheostomy incision. Rigid laryngoscopy showed medialisation of laryngeal structures on the left with mild false cord oedema but no laryngeal mass.
Histological examination of the biopsy showed fibrocollagenous tissue infiltrated by sheets of highly atypical cells with neuroendocrine features. Tumour cells showed positivity for PSA (prostate-specific antigen), PSAP (prostatic specific acid phosphatase), CD56, chromogranin and TTF-1 (thyroid transcription factor 1). The findings were consistent with those of metastatic prostatic carcinoma with neuroendocrine differentiation, similar to the previous histological findings from the prostate.
A multidisciplinary decision was made for palliative treatment due to the extent of disease metastasis.
Distant metastases of cancers are thought to occur via the blood or lymphatic vessels and, as these are sparse within the hyaline thyroid cartilage, prostate cancer metastases to the thyroid cartilage are considered very rare. Indeed, a literature search has revealed only six other reported cases of prostate carcinoma with thyroid cartilage metastasis.1–6
Despite this, a histopathological study has found microscopic metastases to the thyroid cartilage in five out of six postmortem patients with advanced prostate carcinoma, suggesting that distant metastases to cartilage may be more prevalent than previously thought.7 Potential explanations may lie within the haematogenous or lymphatic routes of distant cancer metastases.
First, hyaline cartilage is known to undergo bony metaplasia and ossification during the ageing process and, as bone has a better vascular supply than cartilage, it has already been hypothesised that this phenomenon could explain a distant metastasis through the haematogenous route.8
Furthermore, a recent study has shown that expression of non-caveolar Cav-1 by prostatic carcinoma cells in particular favours lymphangiogenesis. This lymphatic endothelial cell proliferation is mediated by the panangiogenesis regulator, vascular endothelial growth factor-A. A high predilection for lymphatic metastasis can be an early feature of disease progression in prostatic cancer, providing another potential explanation for a very distant metastasis, as seen in this case.9
Learning points
Securing the airway takes priority over other diagnostic tests.
When performing emergency tracheostomy for airway obstruction, where malignancy is highly suspected, consider also performing rigid pharyngoscopy, laryngoscopy or oesophagoscopy and biopsy if time, expertise and facilities permit.
Maintain a wide list of differential diagnoses. A lump in the neck may have metastasised from regions not necessarily above the diaphragm (eg, prostate carcinoma with neck metastasis).
Ethics statements
Patient consent for publication
Acknowledgments
We would like to thank Nicola Brown from the imaging office for assisting in acquiring and formatting the images.
Footnotes
Contributors Author JG played a role in idea conception for the paper, planning, conducting case report, interpreting images, gaining patient consent, acquiring images for publication, drafting the paper, literature search, giving approval for publication and agrees to be accountable for the contents of the paper. Author TM played a role in idea conception for the paper, planning, conducting case report, interpreting images, drafting the paper, literature search, giving approval for publication and agrees to be accountable for the contents of the paper. Senior author MC played a role in idea conception for the paper, planning, conducting case report, interpreting images, drafting the paper, literature search, giving approval for publication and agrees to be accountable for the contents of the paper. All three authors were involved in the management of the patient.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.