Article Text

Statistics from Altmetric.com
Description
A 32-year-old male patient reported to clinic with a chief complaint of pain along with recurrent bouts of bad taste and swelling in the upper front tooth region for a year. Dental history revealed that the patient sustained trauma 10 years ago. On clinical examination, teeth #11 and #21 were tender on percussion without any mobility or periodontal pathosis. A draining sinus tract was present on the buccal attached gingiva of tooth #11. Both teeth #11 and #21 showed no response to electric pulp testing. Since root fracture lines are usually oblique in the buccolingual direction, periapical radiographs were taken from multiple angulations of 45°, 90° and 110°.1 2 Radiograph of tooth #11 revealed a root fracture at the junction of middle and apical third, blunting and loss of lamina dura of the coronal segment and substantial mesial displacement of the apical fragment. Sinus tracing was done in which the gutta percha cone stopped against the apical fragment. There were radiolucencies in relation to the apical fragment of tooth #11, the neoapex of tooth #11 and periapex of tooth #21 suggestive of chronic periapical abscesses (figure 1A). Even though Cone Beam Computed Tomography (CBCT) was not done in this case, it is reported to provide high-quality 3D images which are valuable in detecting root fractures and associated alveolar socket fractures if present.3 The sensitivity of CBCT images for the detection of root fractures is 89.5%, which is much higher than that of radiographs (26.3%).4

(A) Preoperative Intra Oral Peri-Apical radiograph showing the fractured and mesially displaced apical fragment. (B) Working length determination. (C) Postobturation radiograph.
Since the apical fragment was established as a possible proponent of periapical infection, the treatment plan comprised of the endodontic treatment of the coronal segment with an apical barrier using Biodentine followed by surgical removal of the apical fragment on tooth #11 and endodontic treatment on tooth #21. Anaesthesia was achieved using 2% Lignocaine with epinephrine via buccal infiltration. Rubber dam was placed, access cavity preparation was done on teeth #11 and #21. Working lengths were determined (figure 1B). Biomechanical preparation was completed using K files in step-back technique up to apical file size of #60 along with 2.5% sodium hypochlorite and saline for irrigation. Canals were dried and compacted with calcium hydroxide intracanal medicament and the patient was recalled after 1 week. The putty-like Biodentine mix was carried into the root canal with an amalgam carrier and compacted into the apex of #11 using hand pluggers in increments to form an apical plug of 4–5 mm thickness. The remaining root canal was obturated with thermoplasticised gutta percha and the access cavity was restored. Tooth #21 was obturated using cold lateral condensation technique with AH plus sealer (figure 1C).
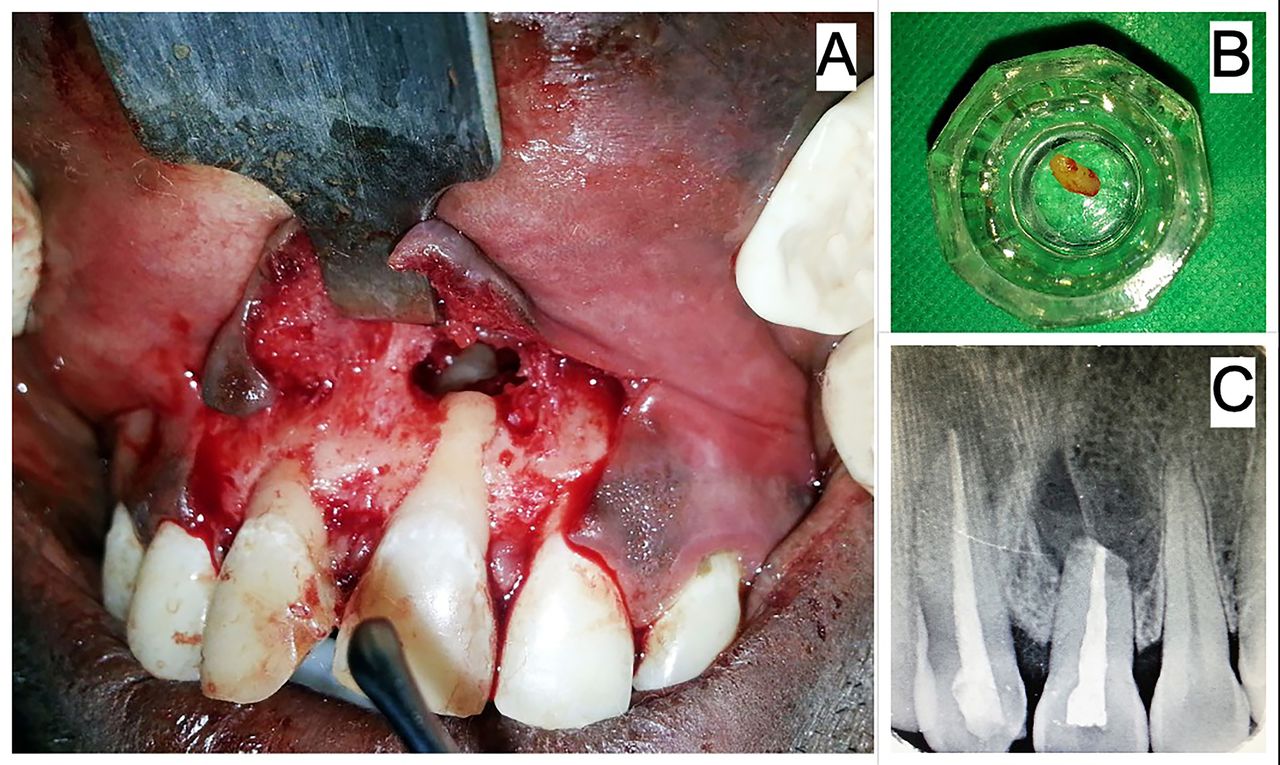
In the following visit after 1 week, apical fragment was surgically removed. Anaesthesia was achieved using 2% lignocaine with epinephrine via buccal infiltration and nasopalatine nerve block. A full thickness mucoperiosteal flap was raised from tooth #22 to tooth #12. The buccal cortical plate in relation to tooth #11 was resorbed. Granulation tissue was curetted to expose the displaced apical fragment (figure 2A). The apical fragment was removed (figure 2B). The bony cavity was debrided and the flap was sutured back. One year follow-up showed complete resolution of symptoms and satisfactory healing (figure 2C).
{kind=link}
{kind=link}
(A) Intraoperative view—raised mucoperiosteal flap revealing depleted buccal cortical plate along with the displaced apical fragment in situ. (B) Fractured apical fragment removed. (C) Follow-up after 1 year showing satisfactory healing.
Patient’s perspective
By the time I approached the dental specialist for my treatment, it was already over a year that I was having issues with my front teeth. I also had pain for which I used to take pain killers. The pus and bad smelling mouth almost prevented me from talking to people normally since I was always anxious about bad breath. I was explained the entire treatment steps thoroughly. The surgery was done after which it healed well and I did not have much discomfort as much as I had anticipated. After the treatment, I was completely free of all the issues I had. It was a great relief from the dirty taste and bad breath bouts. Also, I have been completely pain free since then. I am really thankful to the dental specialist and her team for the exceptional treatment experience.
Learning points
It is important to know that in most cases of infected teeth with fractured roots, only the coronal segment requires endodontic treatment because the pulp in the apical fragment is usually unaffected and does not become necrotic.
In cases of root fractures, it is rare for an apical fragment to get infected; thus, it becomes imperative to diagnose it correctly and provide treatment options which is either root canal treatment of both the coronal segment and the apical fragment or root canal treatment of the coronal segment followed by the surgical removal of the apical fragment, which was done in this case.
Various retrograde root filling materials are used in creation of an apical plug including GIC, MTA, biodentine, bioaggregate, endosequence root repair material among many others.
Ethics statements
Patient consent for publication
Footnotes
Twitter @Drgouravsahu
Contributors LLV was responsible in diagnosis, treatment plan and treatment of patient. AB contributed to treatment and follow-up of patient. GKS contributed in preparing manuscript. SC helped in editing and final proof reading of manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.