Article Text

Statistics from Altmetric.com
Description
A 52-year-old man presented with a slowly growing lump in the neck for 5 years that rapidly extended to the chest wall in the past 6 months. Symptoms and signs of thyroid hyperfunctioning or hypofunctioning were absent. Mechanical compression signs including dysphagia, shortness of breath and hoarseness were not observed. A solid mass around 4 cm in diameter with unclear border was palpated on the left lobe of the thyroid gland. No pain and other inflammatory signs were observed in the thyroid gland. The neck mass moved upward and downward on swallowing. We found prominent extension from inferior pole of the left thyroid lobe downward to the chest wall around 15 cm long (figure 1). Although the extended lesion was a dark purple lesion, tenderness was not found. Palpation revealed firm, tubular, fixed lesion overlying the sternum. Neck lymph nodes were not clinically palpated. CT-scan showed inhomogeneous amorphic lesion around 5.8 cm in diameter with irregular border and multiple internal calcifications in the left thyroid lobe (figure 2). A well-defined, hypodense, non-contrast-enhanced lesion from the left thyroid lobe was found ventrally to the sternum with 21.5 cm long up to the xiphoid process (figure 2). Fine-needle aspiration biopsy revealed follicular lesion of Bethesda class III. Total thyroidectomy and removal of the extended lesion were then performed. Pathological features showed polymorphic cells in papillary arrangement with enlarged round and oval nuclei and coarse chromatin forming a ground glass appearance. Infiltration to thyroid capsule, extrathyroidal adipose tissue and muscles was found. No lymphoid and vascular invasion was observed. The extended lesion was a 20 cm long tubular sac with 4 cm in diameter consisting of fibrous and adipose tissues with small focuses of polymorphic epithelial cancer cells. Radiofrequency ablation using I-131 was administrated 2 months after surgery. The patient was then treated with suppressive treatment of levothyroxine 100 μg/24 hours. Evaluation 6 months after surgery showed serum thyroglobulin was 4.3 ng/mL and thyroid-stimulating hormone was maintained 0.1 mIU/mL. The patient tolerated the treatment well and was able to carry out his daily routine independently and return to his previous levels in the workplace.

Clinical presentation of extrathyroidal extension of thyroid cancer to the ventral sternum.

{kind=link}
{kind=link}
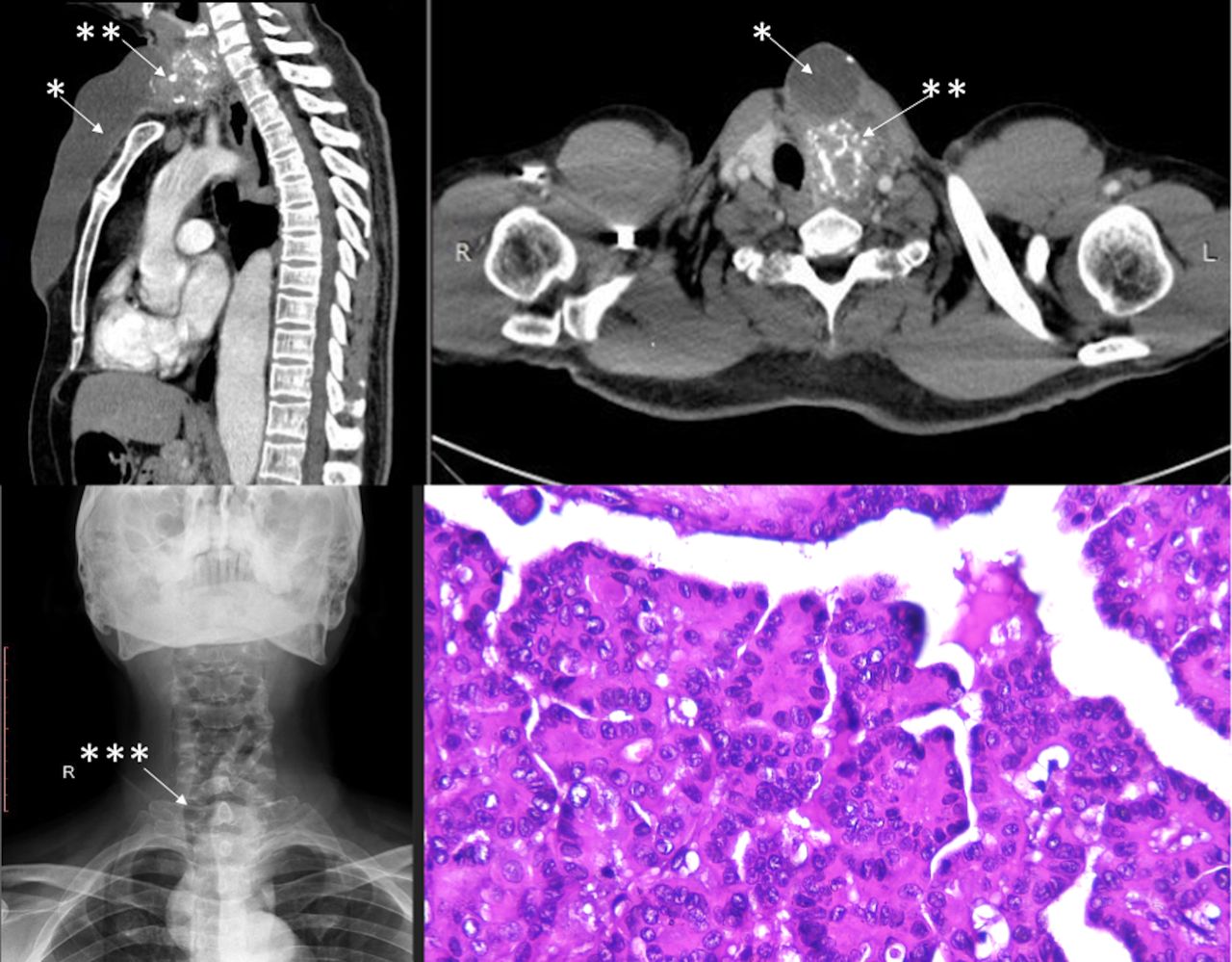
(A) Neck CT-scan demonstrated an inhomogeneous amorphic lesion (*) with irregular border and multiple internal calcifications (**) in the left thyroid lobe. (B) Cervical X-ray showed deviation of the trachea (***) to the contralateral extrathyroidal extension (C) Pathological features showed a classic papillary thyroid carcinoma with ground glass appearance.
Local extension is a common presentation of papillary thyroid carcinoma particularly to central neck lymph nodes and perithyroidal soft tissues.1 2 Invasion to the subcutaneous tissue, larynx, trachea, oesophagus, and recurrent laryngeal nerve was considered as T4 in the Tumor Node Metastasis (TNM) system.1 2 Different from previous reports showing extension to the ventral of thoracic wall,3 4 our case had more rapid period of disease progression. Pathophysiology of sternal extension of thyroid cancer is largely unknown due to limited reported cases. Complete surgical resection including the involved structures of papillary thyroid carcinoma with margin-free potentially results in curative outcome and long-term survival.2 A positive surgical margin is frequently found in T4 papillary thyroid cancer which is associated with poorer prognosis.2 5 Extrathyroidal extension is an independent prognostic marker in papillary thyroid cancer.2 5 6 The presence of extrathyroidal extension, positive lymph node, older age might require more aggressive treatment and intensive surveillance.2
Learning points
Extrathyroidal extension of a papillary thyroid cancer can be manifested as a markedly tubular lesion in the thoracic wall overlying the sternum.
Extrathyroidal extension indicates a high-risk papillary thyroid cancer that might require more intensive treatment and surveillance.
Complete surgical resection involving the infiltrated structures in papillary thyroid cancer is associated with potential curable intent and long-term survival.
Ethics statements
Patient consent for publication
Footnotes
Contributors HH conceived the report, revised and gave feedback to the manuscript. EKD provided expertise in pathology, gave feedback to the manuscript. WSA provided expertise in the imaging, gave feedback to the manuscript. SLA wrote the first draft, revised and coordinated the report.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests All authors declared for no existing competing interest.
Provenance and peer review Not commissioned; externally peer reviewed.