Article Text

Abstract
Vaping may lead to spontaneous pneumothorax, but there are few published reports on this phenomenon. We present a case of vaping-related pneumothorax and make recommendations for structured reporting of this emerging cause for pneumothorax. A normal-weight 34-year-old male presented to our emergency department with dyspnoea and back pain increasing over 24 hours. Chest X-ray showed a large right-sided pneumothorax. Three years ago, he had quit smoking cigarettes and switched to vaping. CT scan revealed bullae, and the patient received apical lung resection. Histology revealed mild alveolitis. Vaping is an emerging cause of lung injury. This report demonstrates a potential association between vaping and pneumothorax. However, structured reporting and future research are needed to establish a definitive (or causal) relationship between vaping and pneumothorax.
- pneumomediastinum
- pneumothorax
- drug misuse (including addiction)
- tobacco-related disease
- cardiothoracic surgery
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- pneumomediastinum
- pneumothorax
- drug misuse (including addiction)
- tobacco-related disease
- cardiothoracic surgery
Background
Vaping devices (electronic cigarettes (e-cigarette)) have gained popularity in recent years. Increased marketing of these devices has been paralleled by reports of e-cigarette or Vaping Product Use-Associated Lung Injury (EVALI),1 life-threatening bronchiolitis (similar to bronchiolitis obliterans or ‘popcorn lung’),2 persistent severe fixed airway obstruction3 and asthma.4 The first regular publication of a case of a vaping-related primary spontaneous pneumothorax (PSP) was published online in September 2019 from Harvard Medical School.5 A case of vaping-related secondary spontaneous pneumothorax (SSP) that was experienced shortly after treatment for vaping-induced pneumonitis was reported in November 2019 from Corpus Christi Medical Center in Texas, USA.6 Before and after these two publications, several conference abstracts of cases of vaping-related pneumothorax have been published.
PSP is a well-known disorder in young otherwise healthy adults that is associated with numerous risk factors. These risk factors include being underweight, lean habitus, scuba diving, high altitude, flying, smoking and, more specifically, smoking cannabis.
Risk factors like being underweight or atmospheric pressure changes generally are accepted as contributing to or causing pneumothorax. However, it is still a matter of debate whether other factors such as smoking cannabis predispose individuals to or otherwise contribute to PSP. One reason for this continuing debate is missing information from case reports and case series.7 8
As this report is now the seventh regular publication about pneumothorax in association with vaping, it is worthwhile considering the information that should be included for such cases and for reviews.
In this study, we used the CARE checklist to report a case of a patient presenting with a pneumothorax associated with vaping without the patient ever consuming cannabis. As we expect further cases to be reported for pneumothorax in relation to vaping, we report our case together with recommendations for standardised reporting of this relationship. In the absence of standardised reporting, drawing a causal link between vaping and PSP will be difficult if not impossible.9 10
Case presentation
In October 2019, a 34-four-year-old white male presented to his general practitioner with a 1-day history of back pain, shortness of breath, tightness in his chest, burning pain in his right chest, retrosternal pain and feeling dizzy. Symptoms started after minor exertion during the afternoon on the day before presentation.
Medical history
No specific health problems occurred during adolescence. His previous medical history was otherwise unremarkable apart from a few rib fractures on his right side sustained through a cycling accident 3 years ago. There was no family history of lung disease. As a trained nurse, the patient worked in outpatient palliative care and devoted his free time to strength training and competitive sports. Due to his occupation, he had regular health checks, all negative for infectious diseases. He had no recent sports trauma to his chest. Despite being an active and internationally successful athlete, he smoked 20 cigarettes per day from the age of 21 years to the age of 31 years. Three years ago, he quit smoking by switching to vaping nicotine. He never smoked or vaped cannabis. He reported a pattern of regular deep and slow inhalation with the vaping device throughout the day similar to smoking a pack of cigarettes.
Clinical findings
On physical examination, we saw an athletic male with normal body mass index (BMI 23.6, 184 cm body height and 80 kg body weight). There were no signs of chronic lung disease such as finger clubbing, chronic cough, wheezing or sputum production. Neurology examination was unremarkable. During the patient’s initial visit to his general practitioner, vitals included a heart rate of 72 beats per minute, blood pressure of 143/91 mm Hg, peripheral oxygen saturation without air supply of 98% and a respiratory frequency of 15 per minute. His ECG demonstrated signs suggestive of myocarditis. The patient arrived at our emergency department 2 hours later with normal peripheral oxygen saturation of 98%, but increasing tachypnoea with 24 breaths per minute. His heart rate and blood pressure remained normal, and there was no enlarged jugular vein pulse or cyanosis. Respiratory frequency returned to normal rates with 3 L of nasal air flow supply. ECG demonstrated again changes in V3–V5 suggestive of myocarditis (figure 1). His skin was dry and warm on palpation with a temperature of 36.8°C, and his tongue was of healthy appearance. His heart sounds were regular on auscultation and breathing sounds were absent on the right side of his chest. Percussion revealed tympanitic chest sounds on the right. The patient complained of acute pain in his chest.
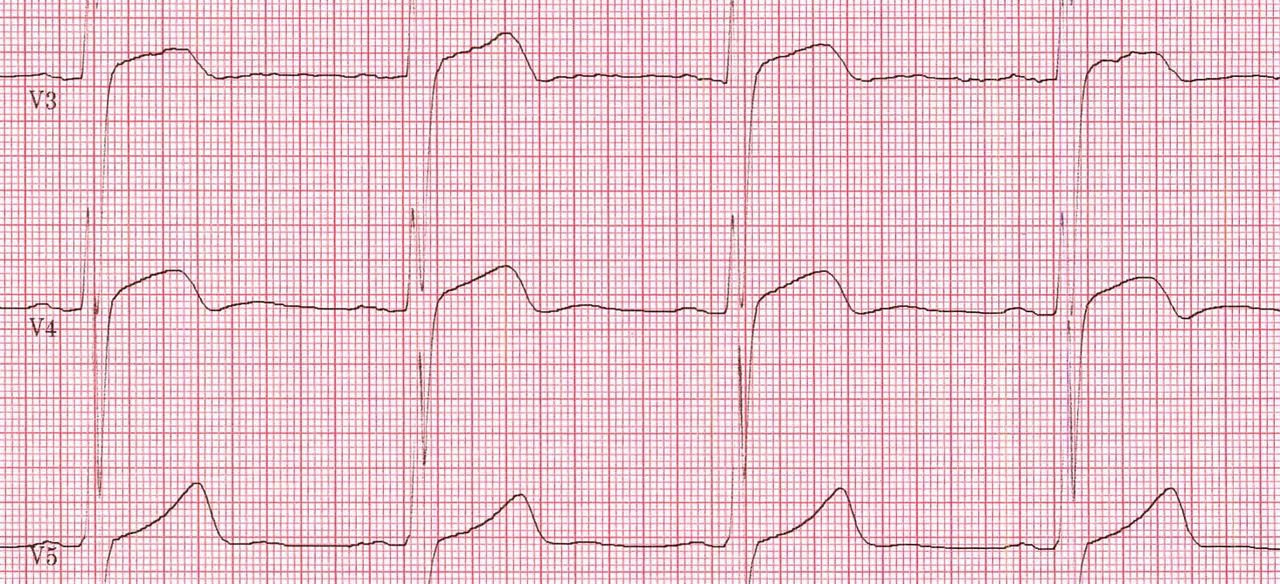
ECG on admission demonstrating ST-elevation in V3–V5 (40 Hz, 50 mm/s, 10 mm/mV).
Diagnostic assessment and therapeutic intervention
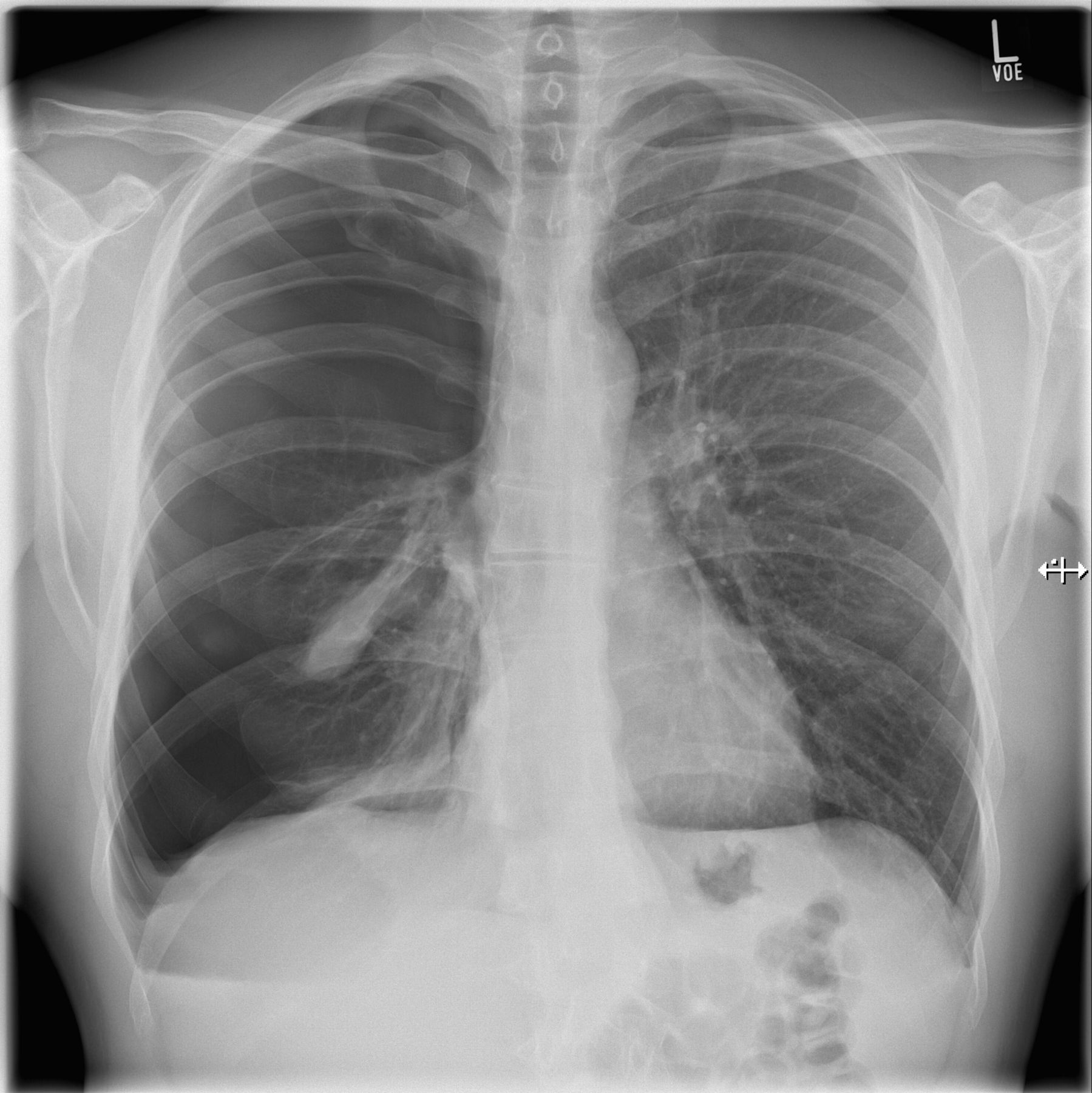
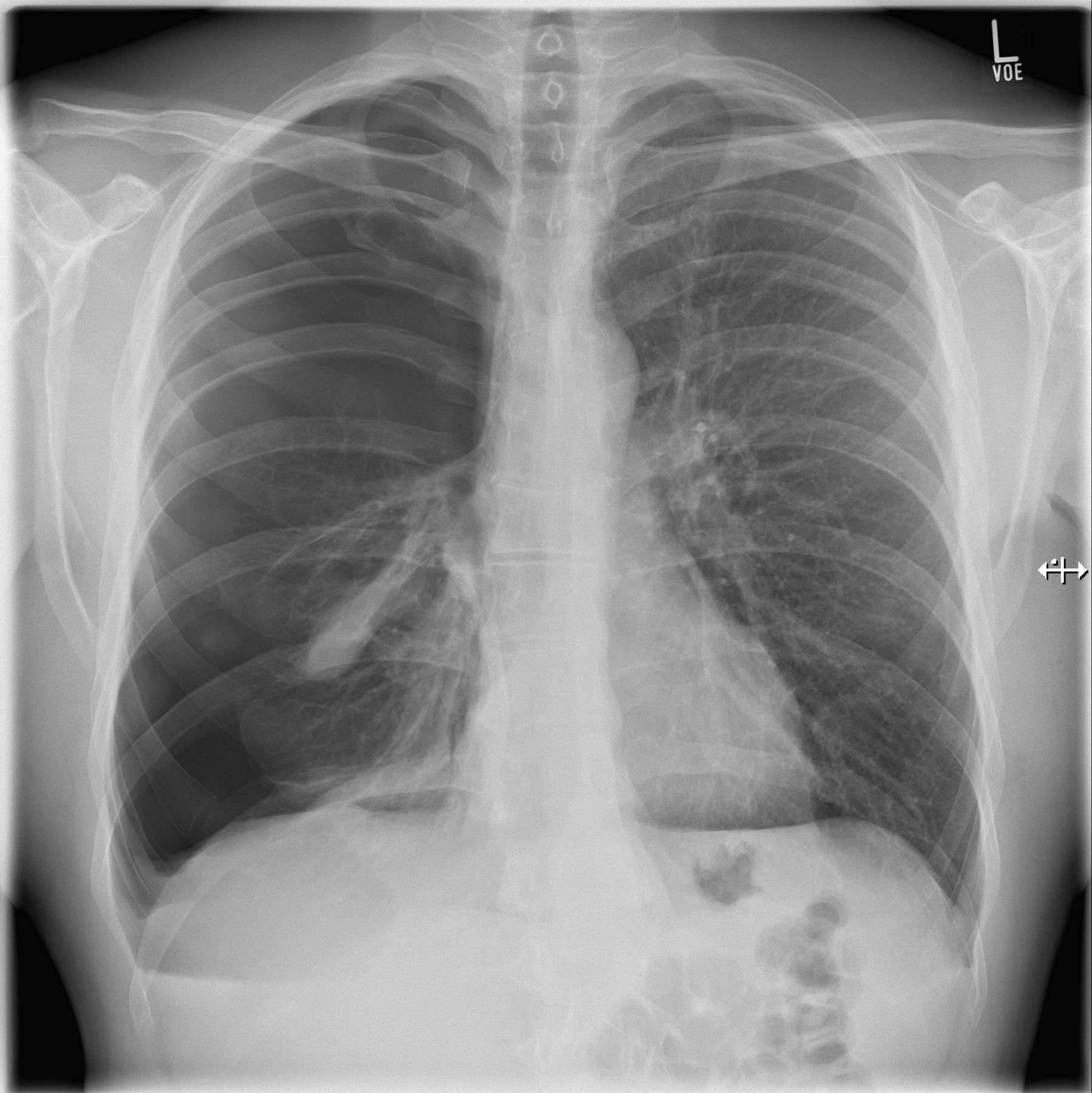
His chest X-ray demonstrated a large (according to Collins formula11) right-sided pneumothorax (figure 2) and a small right-sided pleural effusion. Immediate insertion of a right-sided chest tube led to pain relief and normalisation of the ECG.
{kind=link}
{kind=link}
Posteroanterior chest X-ray in inspiration on presentation, demonstrating a large right-sided pneumothorax.
Diagnostic and therapeutic approaches were discussed with the patient, and a decision was made for a CT thorax scan. The CT scan demonstrated a bilateral inflated lung, the inserted chest tube on the right side, apical bleps of approximately 0.5–1.0 cm in diameter and a small stripe of remaining apical pneumothorax. Blood tests did not reveal any inflammation or other abnormal findings. After successful removal of the chest tube, the patient was discharged and returned for follow-up examination 1 week later in our outpatient department. During the visit, the patient stated his desire to proceed with bullae resection. Being active in martial arts and internationally successful, he feared of another episode of a pneumothorax leading to a further delay in his training.
The patient underwent video-assisted thoracoscopic surgery (VATS) resection of the apical bullae and partial apical pleurectomy. Intraoperatively, the apical bullae and a minor clear fluid collection could be demonstrated with no other visible lung pathology. The resection specimen revealed the site of ruptured bullae. The patient made an uneventful recovery. Perioperatively, the patient received routine tyloxapol inhalations four times daily. Standard analgesia contained oral metamizole, ibuprofen and oxycodone/naloxone.
Outcome and follow-up
After uneventful recovery and chest tube removal, the patient was discharged and re-evaluated 10 days later in the outpatient clinic. The patient reported normal breathing and no need for analgesia. He returned to work 4 weeks after discharge from our care and gradually resumed sports activities 6 weeks after surgery. The patient did not stop using his vaping device during treatment and continued use at follow-up. We invited the patient to review his histology slides under a twin microscope and counselled him regarding chronic health effects of smoking and vaping. He was asked to self-assess his vaping habits with the Self-Report Habit Index (SRHI, German version). While he reported being a frequent vaper, his SRHI score (0.83) suggested only a modest level of habitual use.
Histology
The histology of this resection specimen revealed a subpleural bulla with typical histopathology of a pneumothorax with bulla rupture and small resorbed micro-bleeding. The surrounding lung tissue was characterised by a loss of lung parenchyma and by destruction of alveoli so that there was permanent dilation of airspaces. Large dilated airspaces—bulging from beneath the pleura—were clearly visible. There was also residual lung tissue with mild macrophagocytic alveolitis and signs of mild, chronic, fibrosing inflammation. Hyperdistention of alveolar ducts associated with rupture of alveolar septa was also seen. The specimen did not reveal lipid-laden macrophages.
Vaping device used
The basic anatomy of vaping devices can be found in vaping-related internet content.12 Our patient used an atomiser-type Vapefly Brunhilde MTL RTA 8 mL (MTL—mouth to lung, RTA—rebuildable tank atomiser). The coil used was a Geek Vape Stainless Steel 316 L, 15 wraps with 1.08 Ω, used with 20 W. Wicking for the coil was Wic ‘N’ Vape Cotton Bacon Prime. The Mod (battery carrier) was a VooPoo Drag 2 Box Mod. The vaping device was used with the following e-liquid: Dampfplanet Liquidbase VG50/PG50 (VG—vegetable glycerin, PG—propylene glycol) with Dampfplanet nicotine shot 20 mg/mL without flavour. The e-liquid was mixed with nicotine to achieve a concentration of 6 mg/mL. The patient stated that he uses his vaping device on a daily basis and consumes approximately 16 mL of e-liquid per day.
Analysis of previous case reports and recommendations for reporting
We analysed six previously published case reports and case series5 6 13–16 and several conference abstracts17–25 of pneumothorax in association with vaping. We only analysed reports in English. Information on patient demographics, medical conditions, presenting symptoms, diagnostic findings and outcomes was examined. Results are reported in table 1. Given the relative paucity of data on the relationship between vaping and pneumothorax, we used a tabular evaluation of existing case reports and conference papers. This method has been previously used by DeVito et al.26 In their review, the authors aimed to elucidate the impact of nicotine exposure from vaping devices on addiction and psychiatric symptoms and produced a qualitative table to depict standardised information. Here, we present a similar qualitative table that provides standardised information relevant to the aims of the current case report.
EVALI-associated pneumothorax in relation to demography, complications and treatment
Discussion
We presented a case of a young, healthy athlete who reported daily nicotine vaping and experienced an episode of spontaneous pneumothorax. This pneumothorax likely was a secondary spontaneous pneumothorax based on the presence of emphysematous bullae observed via his CT scan and histology slides. By analysing previous pneumothorax cases with vaping-related lung injury, we found two distinct types of pneumothorax presentation. Sixty per cent of reports analysed through table 1 demonstrated pneumothorax together with the truly horrifying changes of the lung parenchyma on CT scans that marked the EVALI outbreak in the USA with ground glass opacities (GGO), ‘crazy paving patterns’, absurdly large bullae in young people, bronchiectasis and volume loss (ie, the GGO group).27 In contrast, our patient was an athlete presenting with pneumothorax secondary to emphysema due to smoking and vaping nicotine without major structural changes of the lung parenchyma. The last seven cases in table 1 share similar clinical presentation and outcome including our case (ie, the non-GGO group). Chest X-rays and CT thorax scans of these patients did not show any major parenchymal changes together with a pneumothorax. There was no statistically significant age difference between the GGO and the non-GGO groups (27.1 vs 21.4 years, p=0.16). BMI, nutritional status or body habitus of the patients rarely were reported, so we could not examine differences based on these factors. All patients in the non-GGO group were male, their previous medical history was unremarkable and they had no current infection or infectious diseases. Interestingly, although information on vaping duration was not included in seven cases reports, the numbers extracted give the impression that the duration of vaping in the GGO group was rather short compared with the more uncomplicated pneumothorax in the non-GGO group (10.8 vs 21.8 months, p=0.31). The relatively short vaping duration observed in the GGO group is consistent with the presentation of EVALI cases observed during the 2019 outbreak in the USA.
Despite pneumothorax being a major complication of vaping and despite a strong association between smoking cannabis and pneumothorax as well as between vaping and use of cannabis in vaping products, information on cannabis use and toxicology proof was not available for all cases reviewed. In addition, information used to classify pneumothorax (PSP or SSP) like the presence of coughing or thoracic strain was not provided in several reports. Therefore, we reclassified the pneumothoraces into PSP and SSP according to an accepted definition and according to the information given in the reports.28 Only two of the pneumothoraces in the non-GGO group might be regarded as vaping-related primary spontaneous pneumothoraces. Interestingly, none of the patients in the non-GGO group developed bilateral pneumothorax, whereas 5 of 11 patients in the GGO group developed bilateral pneumothorax. In 7 of 11 cases in the GGO group, pneumothorax developed with a latency of 4–18 days after presentation. Furthermore, 4 of 11 patients in the GGO-pneumothorax group needed ECMO support. None of the patients similar to our patient (non-GGO group) developed respiratory failure. In both groups, recurrent pneumothoraces and bronchial fistula occurred. Interestingly, Gonsalves and colleagues reported recurrent pneumothorax after PSP in three out of three EVALI cases.29 Here, we found recurrent pneumothorax after PSP and after SSP in both the GGO and non-GGO groups. In five of the cases reviewed in table 1, no information on pneumothorax management could be retrieved.
Table 2 is a checklist-type table that we created based on previous reviews of EVALI cases and our own experience that may be used to encourage standardised reporting of vaping-related pneumothorax.29–33
Checklist for reporting of vaping-related pneumothorax
Our patient also presented with rather rare ECG changes suggestive of myocarditis. There are few reports of such ECG changes with a right-sided pneumothorax.34 ECG changes resolved quickly after chest tube insertion on the day of admission. Management with VATS resection of the right lung apex was successful, and the patient restarted training in martial arts 6 weeks after the operation. Histology of the lung specimen revealed typical pathology of nicotine smoking-related pneumothorax. No specific investigations are known for pathology specimens from vaping-associated pneumothorax.
The patient demonstrated in-depth knowledge of his vaping device and reported that it helped him to quit smoking 3 years ago. Prior to switching to vaping, the patient smoked approximately 20 cigarettes per day for a period of 10 years despite being a successful athlete. The patient reported his athletic ability increased after switching to vaping. The patient was well aware that, in the long term, there might be significant changes to his fitness due to structural changes in his lungs and vessels. The patient clearly understood that vaping nicotine might help quit smoking nicotine but might not lead to a decreased spectrum of related illnesses.
As was the case with smoking, it likely will be decades after the introduction of e-cigarettes until the full picture regarding associations between vaping and diseases emerges. The current report is only the seventh case report to highlight vaping-related pneumothorax. However, pneumothorax in young adults has been strongly associated with cigarette smoking and cannabis use; case–control studies have established both as significant risk factors for pneumothorax.35 Yet, evidence of a causal relationship is lacking. Moreover, whole case series of vaping-related lung injury have been published without any patient experiencing a pneumothorax.32 36 Compared with this report, Jonas et al identified 8 patients with pneumothorax among 216 published cases with vaping-associated lung injury.31 In 2019, research has, for the first time, tried to identify cannabinoids in lung tissue of young adults with pneumothorax.7 While this is an important step in understanding the relationship between cannabis use and pneumothorax, evidence of cannabinoids in lung tissue does not provide proof of a pathology mechanism. Similarly, it might be difficult to establish a causal relationship between vaping and pneumothorax. However, if such a relationship exists, we expect to see a rise in cases of pneumothorax that accompanies the increased popularity of vaping. Building on the evidence of a cannabis–pneumothorax association, we provided recommendations through table 2 about reporting vaping-associated pneumothorax. As no systematic pathology examination of lung tissue from patients with vaping-associated pneumothorax exists today, there should be an international agreement on what to look for in such specimens.
The mechanism of developing a pneumothorax with vaping is likely to be complex. A factor that has long been suspected of contributing to pneumothorax is inhalation technique. Of note, inhalation technique is one of the main differences between smoking tobacco cigarettes, smoking cannabis and vaping. The importance of researching variation in inhalation technique is underscored by the results of a study on ‘dripping and e-cigarettes’ from Yale University School of Medicine.37 Dr Krishnan-Sarin and colleagues describe that, among 1080 (main sample n=7045) students from eight Connecticut high schools, 282 students (mean age, 16.4 years) used dripping. Dripping is a technique where e-liquids are vaporised directly via application to the atomiser coil to produce a stronger flavour, thicker cloud of vapour and a ‘stronger throat hit’. Dripping can lead to inhalation of higher temperature vapour and exposure to non-nicotinic toxic byproducts such as volatile aldehydes (formaldehyde) in toxic concentrations. Therefore, it is strongly recommended to ask patients about inhalation technique to understand the development of vaping-associated pneumothorax.
A major criticism in reporting of cannabis-related and smoking-related pneumothorax has been the absence of standardised information about smoking habits in case reports and cohort studies.31 32 38 39 Recognising similar problems in addiction research, the European Centre for Drugs and Drug Addiction (EMCDDA) recommended the use of standard questionnaires in 2002.40 The EMCDDA questionnaire has been used in a large Danish cohort study to establish cannabis as a risk factor for PSP,35 but the EMCDDA questionnaire has not yet been updated to include assessments of e-cigarette use. Until psychometrically sound measures of e-cigarette use are included in large, standardised surveys like the EMCDDA, it is critical to source reliable and valid measures of e-cigarette use and related behaviours elsewhere. In this study, we used the SRHI, a recently validated measure of habitual e-cigarette use.41 To increase the scientific rigour and interpretability of findings related to e-cigarette use, the use of validated measures like the SRHI is strongly recommended.
Patient’s perspective
People are likely to think about lifestyle factors contributing to a dramatic episode of illness and hospitalisation while recovering. After reading a lot and asking myself questions, it is still difficult for me to decide whether there is an association between my vaping and experiencing an episode of recurrent pneumothorax. If there is, how are we going to find out the most important contributing factors? There are a wide variety of flavours, mixing ratios of VG and PG and nicotine concentrations in the e-liquid. Moreover, there are different metals used for the coils, energy settings and inhalation techniques. These multiple factors might render it impossible to estimate any correlation between vaping and pneumothorax. Generally, I am very grateful for having my vaping devices as it helped me quit smoking. Currently in my opinion, smoking is still much more harmful than vaping. Taking my occupation as a palliative care nurse into account, this episode with a pneumothorax sharpened my existing views of risks of daily life. One should live the life he wants to live and should enjoy what he wants to enjoy. To know about risks is absolutely worthwhile for making informed decisions, but quality of life is very individual and important too.
Learning points
Vaping nicotine may cause pneumothorax.
For patients with pneumothorax and a background of vaping, ask about inhalation technique and e-liquids used.
Ask for vaping habits using, for example, the Self-Habit Reporting Index.
Counsel for vaping-related health effects.
Ethics statements
Patient consent for publication
References
Footnotes
Contributors DHB provided surgical service to the patient reported here, HK provided respiratory medicine support and counselling services to the patient and supervised reporting of the case, MM first advised on psychometric testing of the patient and than co-wrote and corrected the case report including discussion of requirements from the reviewers and AT performed extensive testing of the lung specimen resected. AT was involved as a champion in lung pathology and advised on writing of the report.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.