Article Text

Abstract
Stent graft collapse due to aortic dissection is an extremely rare event. Although endovascular aneurysm repair (EVAR) and thoracic endovascular aortic repair (TEVAR) are increasingly being performed, various complications can occur. We report a case of collapse of a stent graft, which was used to repair an abdominal aortic aneurysm (AAA) after TEVAR for thoracic aortic aneurysm (TAA). A 72-year-old man with a 77 mm AAA and 60 mm TAA underwent EVAR and a TEVAR 2 months later, respectively. CT performed after the TEVAR showed thoracic aorta dissection with associated AAA stent graft collapse. The graft collapsed was due to superior mesenteric artery obstruction. An emergency TEVAR was performed, and the procedure improved the collapsed graft; however, the endoleak of the AAA stent graft persisted. The AAA expanded over several days, warranting an open repair. Our case provides an insight into the cautionary indications for endovascular therapy.
- interventional cardiology
- cardiothoracic surgery
- vascular surgery
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
In recent decades, thoracic endovascular aortic repair (TEVAR) and endovascular aneurysm repair (EVAR) have become accepted alternatives to open surgery to treat thoracic and abdominal aortic aneurysms.1 However, an increasing number of complications have been reported with the increasing use of endovascular interventions.2 Of these complications, collapse of a stent graft secondary to aortic dissection is an extremely rare event.3 4 Herein, we report a case of collapse of a stent graft, which was used to treat an abdominal aortic aneurysm (AAA) after TEVAR for a thoracic aortic aneurysm (TAA).
Case presentation
A 72-year-old man was found to have incidental findings of a 77 mm AAA and a 60 mm TAA. His medical history included hypertension and hyperlipidaemia. The AAA and TAA were suitable for EVAR and TEVAR, according to the anatomical indications of the procedures. He underwent EVAR for the 77 mm AAA, which was performed using the Endurant system (Medtronic Vascular, Inc., Minneapolis, MN, USA). During the EVAR, the 60 mm TAA was observed, which was treated using TEVAR, 2 months after the EVAR, using the Valiant system (Medtronic Vascular, Inc.). The patient had no complaints following the TEVAR but developed nausea on post-TEVAR day 1.
Investigations
CT revealed a dissection of the descending thoracic aorta, with a collapse of the stent graft in the AAA (figure 1A–D) and a secondary obstruction of the superior mesenteric artery (SMA; figure 1B). This collapse of the AAA stent was considered to have been caused by a stent graft-induced new entry (SINE), which resulted in a type 1b endoleak after TEVAR. The decreased blood flow through the SMA was caused by the collapse of the AAA stent graft.
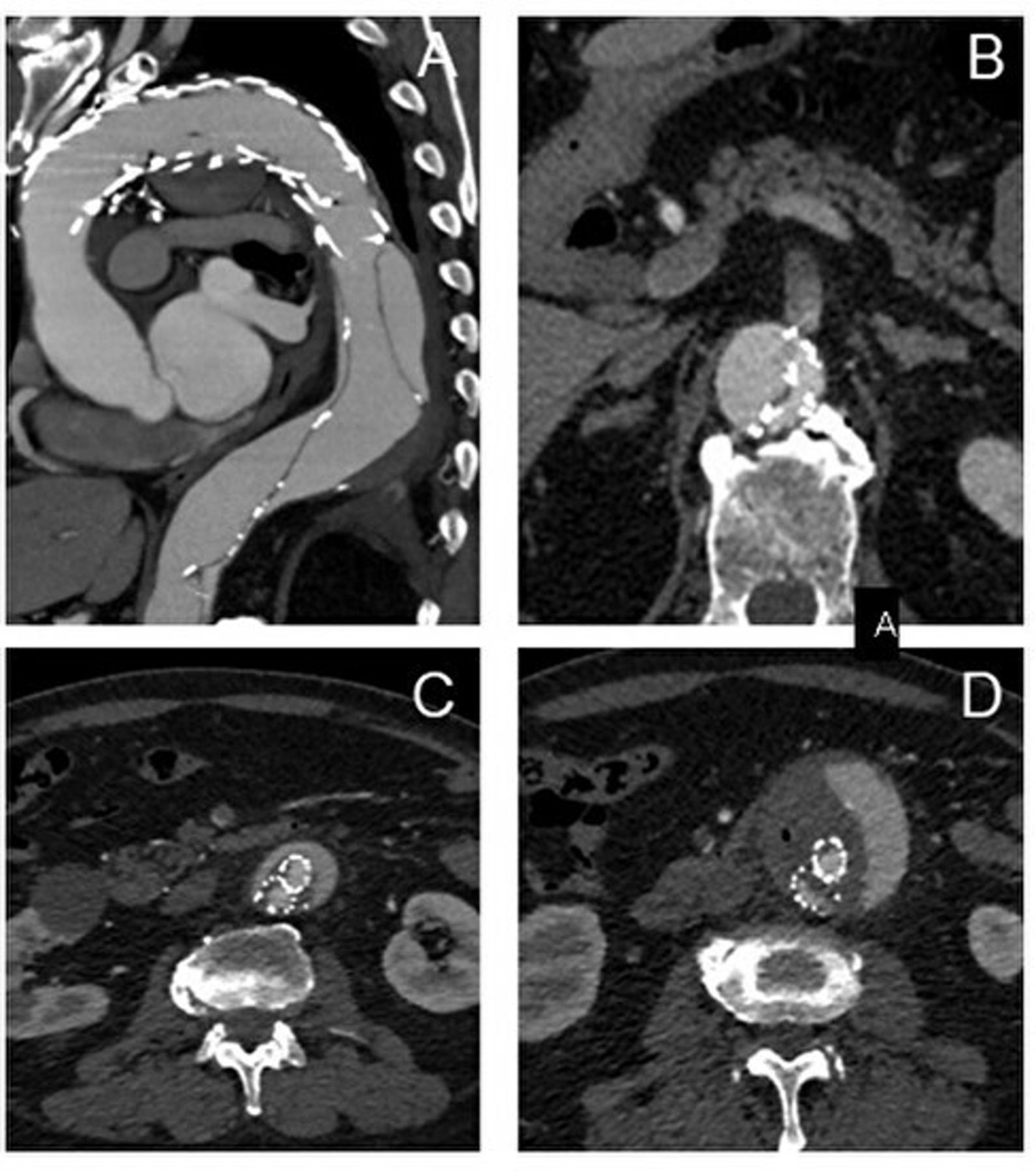
CT images of the aorta 1 day after TEVAR for the thoracic aortic aneurysm (A): dissection of the descending thoracic aorta, which was considered to be caused by a stent graft induced new entry. (B): the collapsed stent graft in the abdominal aortic aneurysm (AAA) with obstruction of the superior mesenteric artery. (C–D): the endoleak in the AAA.
Treatment
Decreased SMA blood flow was an indication for an emergency TEVAR, performed close to the entry of the artery, using a Conformable GORE thoracic endoprosthesis (CTAG; W.L. Gore & Associates, Flagstaff, AZ, USA). The TEVAR resolved the type 1b endoleak, and improvement of the collapsed stent and SMA blood flow was observed on postoperative CT (figure 2A,B). However, the endoleak of the AAA stent graft persisted (figure 2C,D). Because of the persistent endoleak of the AAA stent graft, the AAA expanded for several days (figure 3A), with convexity on the ventral side, an easy-to-rupture form of AAA, which warranted an open repair (figure 3B). For this repair, an Endurant stent graft was inserted in the infrarenal abdominal aorta and both the common iliac arteries, followed by proximal anastomosis—performed using an 18×10 mm Gelsoft graft (Vascutek, Renfrewshire, Scotland); the Endurant stent graft was subsequently cut between the infrarenal abdominal aorta and the common iliac arteries. The Endurant stent graft was then easily removed from the common iliac arteries, allowing distal anastomosis to be performed.
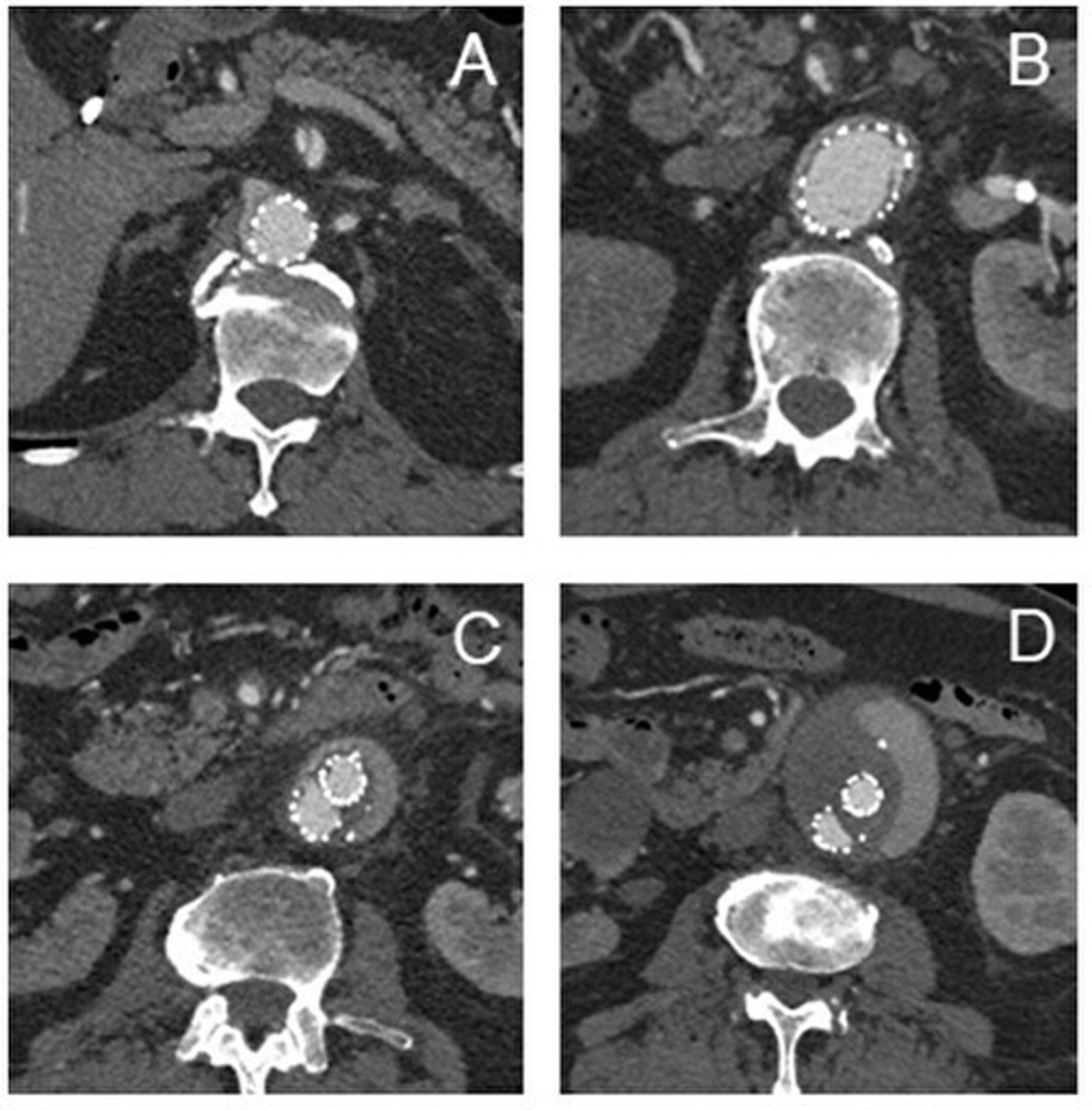
CT images of the aorta after emergency TEVAR. (A) Despite a dissection of the superior mesenteric artery (SMA), an improvement is seen in the blood flow through the SMA after the emergency TEVAR. (B) improvement in the diameter of the collapsed stent graft in the abdominal aortic aneurysm (AAA) after emergency TEVAR. (C–D) The persistent endoleak of the AAA stent graft.

{kind=link}
{kind=link}
{kind=link}
Preoperative CT image and associated surgical findings of the abdominal aortic aneurysm (AAA). The white arrow shows the easy-to-rupture AAA, which is partially convex on the ventral side.
Outcome and follow-up
The postoperative course was uneventful, and the patient was discharged 11 days after the open AAA repair. He was energetic during his follow-up visit 2 years after discharge, and no recurrence of endoleak or aortic dissection was observed.
Discussion
The complications of endovascular therapy, such as EVAR and TEVAR, are diverse and range from mild to severe.5 Major complications include endoleaks (14.6%–16.8%), migration (0.1%), graft limb occlusion (0.9%–4.7%), stent graft infection (0.6%) and SINE (3.4%).6 In particular, SINE, defined as a new tear caused by a stent graft, can be a serious complication, often requiring immediate intervention. In our case, there were no obvious findings suggestive of SINE on angiography examination immediately after TEVAR for TAA, and the patient did not report any immediate symptoms. However, as nausea, which developed on post-TEVAR day 1, did not improve, we proceeded with a CT examination. An emergency TEVAR was performed because of the malperfusion of the SMA due to compression of the true stent graft lumen by a false lumen. The entry tear was detected distal to the stent graft in the TAA, with the patient presenting with symptoms of SMA obstruction requiring prompt revascularisation. Previous reports have reported the efficacy of entry closure using a stent graft in cases of complicated type B aortic dissection.4 7 However, although TEVAR was effective in managing the type 1b endoleak of the TAA as well as improving the collapse of the stent graft placed in the AAA and the blood flow through the SMA, the endoleak of the AAA stent graft persisted, leading to progression of the AAA to an easy-to-rupture status that required additional treatment. We considered EVAR, such as using an aortic extender as a management for the progressing AAA. However, as the stent graft in the AAA was placed just below the left renal artery, additional EVAR was not expected to effectively manage the endoleak of the AAA stent graft. A study assessing the outcome following a conversion from endovascular to open repair was published, and the conversion rate was 1.2%.8 Zeng et al reported that combined TEVAR and EVAR could be performed safely when anatomically feasible, with minimal morbidity and mortality.9 Therefore, TEVAR and EVAR can be considered acceptable alternatives for the treatment of TAA and AAA. Xanthopoulos et al reported that endovascular repair might be an acceptable alternative to open or hybrid surgery to treat coexisting descending thoracic and abdominal aortic pathologies, at least for high-risk patients.10
Endovascular therapy is an effective treatment for thoracic and abdominal aortic aneurysms. However, open repair may be required when evolving conditions require reintervention. Open repair may also need to be considered when endovascular therapy cannot be adapted to the local anatomy, as in our patient.
Patient’s perspective
Around the spring of 2019, at the hospital, I was found to have AAA and TAA. I was in despair. I had no symptoms. My investigations revealed that AAA and TAA could be fatal. However, I was relieved when my doctor explained that both AAA and TAA could be treated by endovascular therapy instead of open surgery. I am scared of surgery, but I did not think endovascular therapy was scary. As I had expected, AAA repair finished in an hour. The length of hospital stay was 3 days. I believed that TAA repair would also be safe and easy.
In the summer of 2019, I underwent TEVAR for TAA repair. Like EVAR, TEVAR was easily completed, but the next day nausea appeared. I had never experienced that kind of nausea before, and it did not improve despite taking medications. On CT, a dissection was found, and I was urgently posted for reintervention. My nausea improved immediately after this treatment. But, when I found out that the AAA was getting bigger on the CT, I was disappointed and thought I might die. I did not want to die, so I agreed to have open surgery. The pain was severe after the operation, but I was able to walk immediately. After the surgery, I found that I was completely cured, and I am able to live my daily life with peace of mind. I heard that it is a rare complication, but I am happy to live a healthy life. I am glad I had the open surgery.
Learning points
We describe a rare case in which thoracic endovascular aortic repair (TEVAR) was successfully performed to treat a collapsed stent graft in abdominal aortic aneurysm (AAA), although open AAA repair was needed later.
Although endovascular therapy, including endovascular aneurysm repair and TEVAR, is increasingly being performed, various complications have been reported.
Our case provides an insight into cautionary indications for endovascular therapy.
Ethics statements
Patient consent for publication
Footnotes
Contributors ST wrote the manuscript. ST and YG treated patient and performed the operation. ST, AN, JY and YG performed the follow-up of the patient. ST and YG performed total organisation of writing the manuscript. All authors read and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.