Article Text

Statistics from Altmetric.com
Description
A 78-year-old woman athlete presented with malaise and right flank pain. Her medical history was significant for well-controlled hypertension, a duplex collecting system (complete ureteral duplication on the right kidney and partial duplication down to just above the ureterovesical junction on the left kidney), ureteral strictures from prior radiation for uterine cancer, total hysterectomy, right-sided hydronephrosis and recurrent bilateral nephrolithiasis. She required numerous laser lithotripsies and ureteral stents. At presentation, vitals were unremarkable. Notable laboratory values included: haemoglobin 7.8 g/dL (11.6–15.0 g/dL), bicarbonate 11 mmol/L (22–29 mmol/L), phosphorus 6.4 mg/dL (2.5–4.5 mg/dL), blood urea nitrogen 75 mg/dL (6–21 mg/dL), serum creatinine (sCr) 4.27 mg/dL (reference range: 0.59–1.04 mg/dL) and estimated glomerular filtration rate (eGFR) <15 mL/min/BSA. There was no leucocytosis. The patient’s baseline sCr was 1.9 mg/dL before 1 month. The urology service performed a cystoscopy with bilateral retrograde pyelogram, which identified severe ureteral strictures involving the mid to distal ureters of both upper and lower pole moieties of the right kidney. There was hydronephrosis in the respective areas. Purulent and cloudy urine was visualised. Unfortunately, there was fibrosis-associated extrinsic compression of prior stents that required a right ureteral dilation. Additionally, two percutaneous nephrostomy tubes were placed in both moieties of the right kidney (figure 1). The left kidney contained several nonobstructive stones in bilateral pole moieties. It appeared grossly normal in size and contour. Due to a rapid decline in eGFR, the nephrology department was consulted, who pursued with a kidney biopsy. The procedure was performed on the left kidney to evaluate for other causes of medical renal disease. There was no evidence of primary glomerular disease via light microscopy, electron microscopy and immunofluorescence. However, eight of the sixteen sampled glomeruli were globally sclerosed. There were abundant calcium oxalate crystals in the tubules with mild tubular atrophy and interstitial fibrosis (5% of the renal parenchyma) (figure 2). Fortunately, with urologic interventions and dietary education, the patient’s sCr improved to 2.35 mg/dL with eGFR of 15–20 mL/min/BSA. Postoperative antibiotics were not needed, as the patient’s clinical status improved after fixing the urologic obstruction. The patient is currently receiving nephrostomy tube exchanges every 6–12 weeks.

Nephrostogram; patient in prone position: right upper moiety demonstrates long segment of stenosis in the distal third of the ureter with sluggish clearance of contrast. Right lower pole moiety demonstrates obstruction of the ureter at the level of the renal pelvis without clearance of contrast.

{kind=link}
{kind=link}
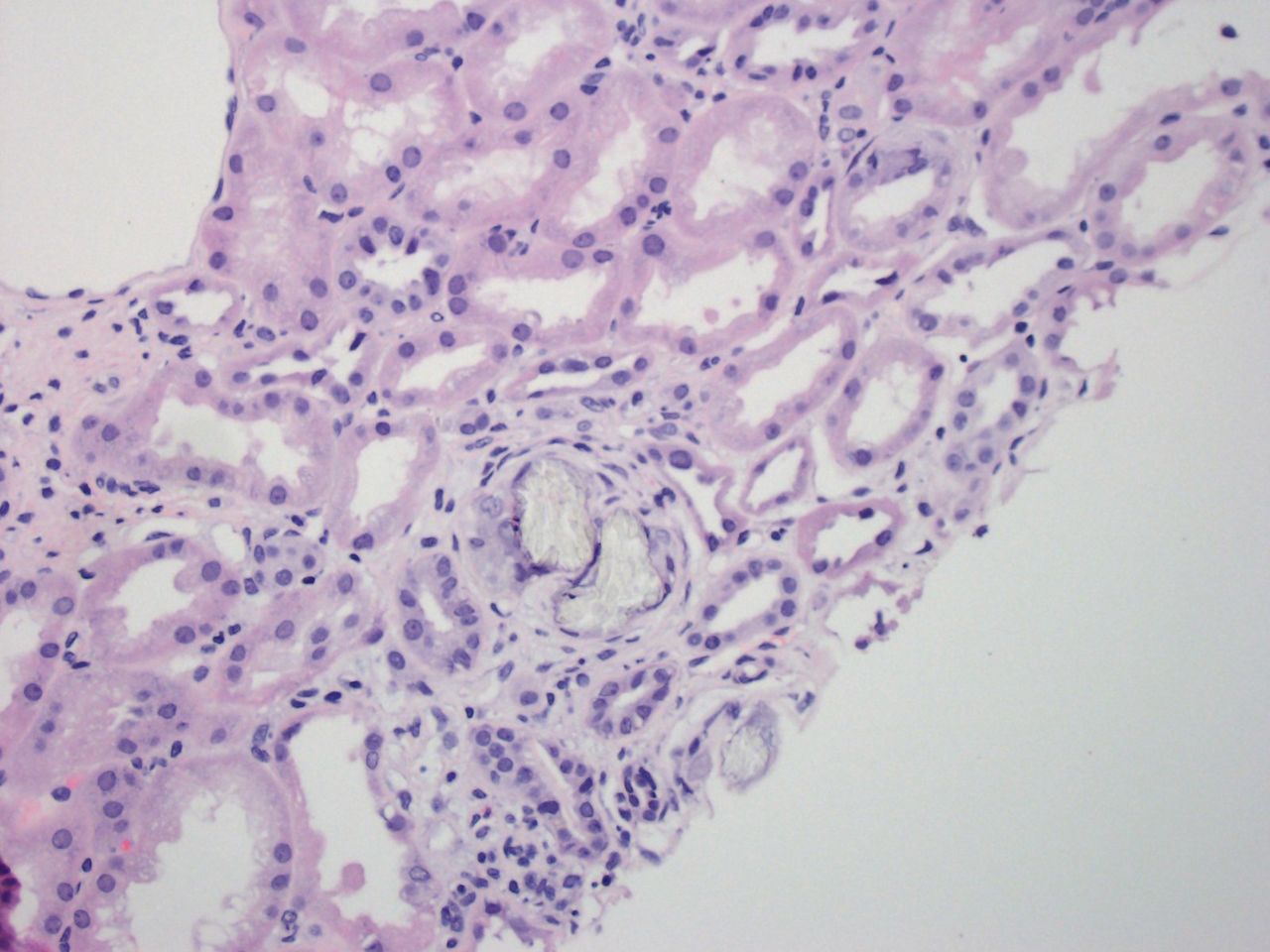
Light microscopy—H&E stain 200×—calcium oxalate crystals within the tubular lumen of the kidney. The crystals are clear and have a fan-shaped appearance. There is mild tubular atrophy and interstitial fibrosis (5% of the parenchyma). There is mild arteriolar hyalinisation.
Secondary oxalate nephropathy can lead to acute kidney injury and chronic kidney disease.1 Our patient was predisposed to oxalate nephropathy and nephrolithiasis due to urologic obstruction. We suspect that her tortuous and fibrotic ureters from a duplex collecting system and prior radiation increased stagnant and supersaturated urine, which fostered crystalluria.2–7 Decreases in eGFR from obstruction increase time of interaction between the crystals and renal parenchyma.6–8 Microscopic crystals activate the NLRP3 inflammasome with subsequent generation of reactive oxygen species, tubular epithelial cell necroptosis and interstitial fibrosis. Damaged renal tubules serve as niduses for further crystallisation and stone formation.5 6 Whereas secondary oxalate nephropathy is mostly caused by excessive dietary oxalate intake, dehydration and intestinal malabsorption, it is important to consider urologic obstruction and anatomical anomalies of the collecting system as potentiating factors.9–11
Learning points
Oxalate nephropathy typically presents as acute on chronic kidney injury or acute kidney injury.
Common precipitating factors of secondary oxalate nephropathy include increased intake of oxalate precursors, intestinal malabsorption, and inadequate hydration. Obstructive uropathy in the setting of a duplex collecting system and ureteral fibrosis can also predispose a patient to this condition.
Ethics statements
Patient consent for publication
Footnotes
Contributors IEP conceived the presented idea and conducted the study. AB, CC and IEP collected and interpreted the data. AB wrote the manuscript in consultation with CC and IEP.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.