Article Text

Abstract
A pituitary abscess is a rare intrasellar infection. Correct identification can be challenging preoperatively given its non-specific symptoms and imaging findings. We report a case of a young woman presenting with secondary amenorrhea, visual field deficits and a 2.6 cm pituitary lesion diagnosed to be a craniopharyngioma. A concomitant unexpected pituitary abscess was diagnosed intraoperatively without associated meningeal symptoms.
- endocrine system
- infections
- pituitary disorders
- headache (including migraines)
- neuroendocrinology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Pituitary abscess is an uncommon lesion in the pituitary, accounting for <1% of all pituitary lesions. In most cases, it is uncertain what the exact pathogen is, with treatment entailing both surgical and antibiotic therapies. Although clinical symptoms are non-specific compared with other pituitary lesions, pituitary abscess can be life-threatening. However, presurgical diagnosis is challenging due to the non-specific nature of presenting symptoms, non-specific imaging findings, and the rarity of the disease. We report a patient with a pituitary abscess that was discovered during surgery for a known enlarging pituitary lesion that caused visual deficits and headaches.
Case presentation
A 36-year-old caucasian woman presented to the endocrinology clinic for a preoperative evaluation of an enlarging pituitary lesion. She had a medical history of ankylosing spondylitis previously managed on immune modulating therapy but had stopped 1 year prior to presentation. Two years prior, she was diagnosed with a pituitary macroadenoma during an evaluation of secondary amenorrhea. Biochemical evaluation was negative for hypersecretion but did reveal secondary hypothyroidism: thyrotropin (TSH) 0.789 uIU/mL (normal 0.27–4.2), free thyroxine (FT4) 0.75 ng/dL (normal 0.93–1.7), follicle stimulating hormone (FSH) 2.9 mIU/mL (normal follicular phase 3.5–12.5, ovulation phase 4.7–21.5), luteinising hormone (LH) 2.44 mIU/mL (normal follicular phase 2.4–12.6, ovulation phase 14.0–95.6), estradiol<5.0 pg/mL (normal follicular phase 12.4–233, ovulation phase 41.0–398). Visual field exam at that time was unremarkable. A pituitary MRI showed a 1.9 cm lesion with cystic features, suggestive of a cystic adenoma. The patient was subsequently lost to follow-up until she presented again complaining of worsening vision, headaches and weight loss. She had been in her usual state of health until about 6 months prior to presentation when she developed acute worsening of her chronic headaches followed by unintentional weight loss of 30 pounds over 6 months. The patient denied recent illness or fevers. Repeat pituitary MRI at this time revealed interval growth of the lesion to 2.6 cm with a new signal intensity in the cystic cavity suggestive of haemorrhage and compression of the optic chiasm (figure 1).
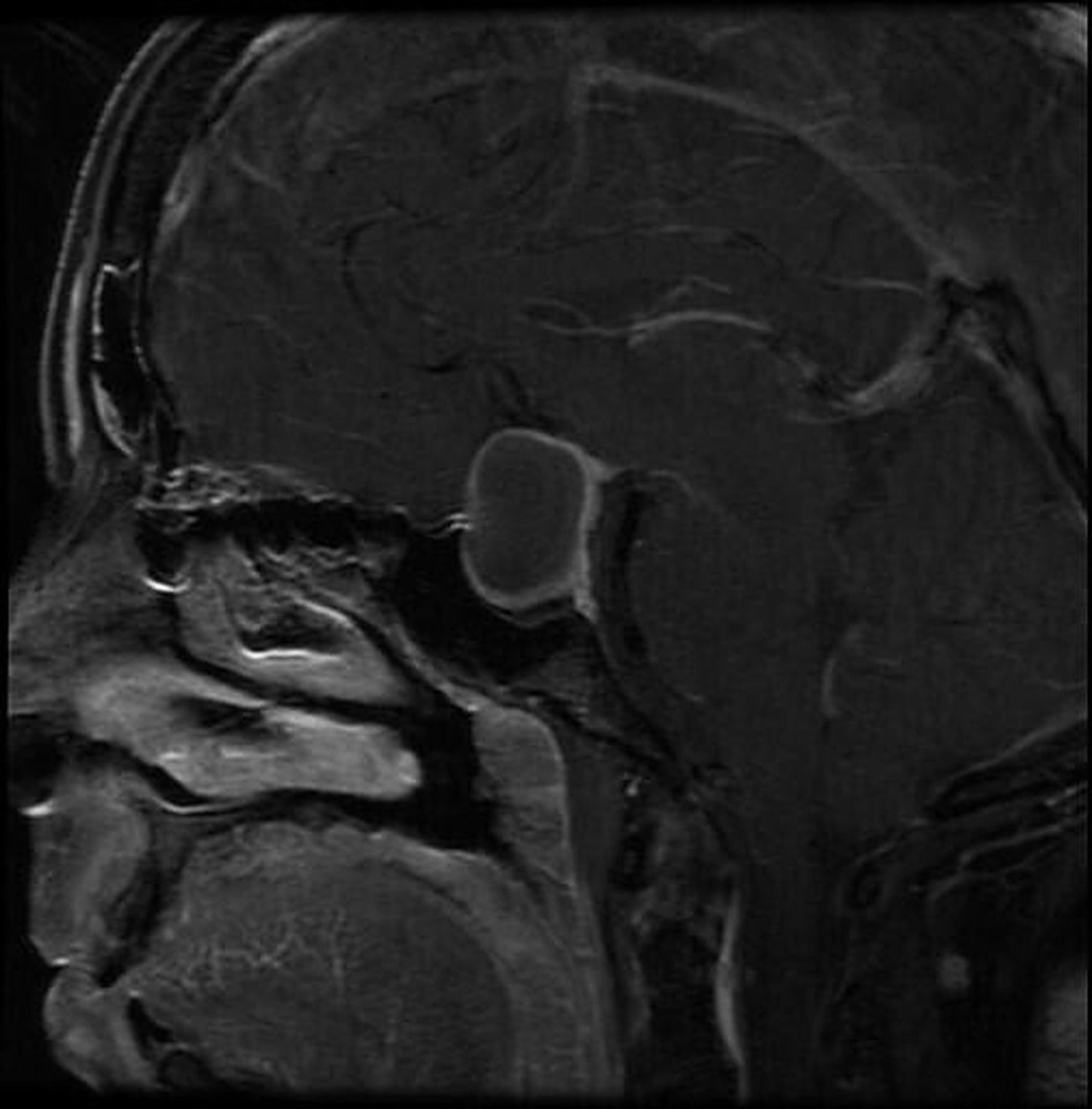
Preoperative pituitary MRI shows a rim-enhancing 2.6 cm lesion with a new signal intensity in the cystic cavity suggestive of haemorrhage and compression of the optic chiasm, which had enlarged from 1.9 cm on prior imaging.
On examination, she was hemodynamically stable and afebrile (blood pressure 116/82 mm Hg, heart rate 74 bpm, respiratory rate 16, oxygen saturation 100% room air and temperature 97○F). Formal visual field testing revealed bitemporal hemianopsia. Laboratory evaluation was negative for leucocytosis but revealed a low morning serum cortisol of 3.0 μg/dL (normal>10) consistent with preoperative adrenal insufficiency. Insulin-like growth factor 1 (IGF-1) level was low at 61 ng/mL (normal 79–259), but an FT4 level was normal on levothyroxine for her known secondary hypothyroidism. Surgical excision of the mass revealed unexpected purulent fluid with culture growing Staphylococcus epidermidis. Histology revealed fragments of non-keratinised squamous epithelium with acute inflammation and papillae in the background of haemorrhage, fibrosis and compressed pituitary gland (figure 2). Chromogranin was negative in the squamous epithelium but reactive in the pituitary gland. TTF1 staining is negative, beta-catenin is strongly positive and BRAF V600E is positive. These findings confirmed a craniopharyngioma.

Histopathology of the lesion shows the squamous cells with marked acute inflammation. In the centre (red arrow), there are blood-filled fibrovascular cores, indicating papillae.
Following surgery, the patient was initiated on broad spectrum antibiotics for 8 weeks. She was initially treated with vancomycin, metronidazole, and ceftriaxone before transitioning to daptomycin and ertapenem as an outpatient. She was placed on physiologic hydrocortisone in addition to maintaining preoperative levothyroxine dose. After 8 weeks of antibiotic therapy, repeat evaluation demonstrated recovery of adrenal axis (peak stimulated serum cortisol 18.1 μg/dL, adrenocorticotropic hormone 39.2 pg/mL (normal 7.2–63.3)) and normalised IGF-1 level.
Three months postoperatively, her visual deficit, weight loss, headaches and adrenal insufficiency resolved, but the previously diagnosed secondary hypogonadism and hypothyroidism persisted. Postoperative laboratory findings showed prolactin 13.9 ng/mL, FSH 3.6 mIU/mL, LH 2.01 mIU/mL and estradiol<5.0 pg/mL (table 1). Pituitary MRI (3 months postoperatively) revealed resolution of rim-enhancing lesion/collection within the sellar/suprasellar region without features concerning for infection (figure 3).
Laboratory findings before and after surgery

{kind=link}
{kind=link}
{kind=link}
Postoperative pituitary MRI shows resolution of rim-enhancing lesion/collection within the selllar/suprasellar region without features concerning for infection.
Discussion
This case report presents a woman diagnosed with a pituitary abscess discovered during surgery for a cystic pituitary adenoma with haemorrhagic features. Differential diagnosis of cystic pituitary lesions includes cystic pituitary adenoma, craniopharyngioma, Rathke’s cleft cyst. Pituitary abscesses are rare, representing<1% of pituitary lesions, with 300 cases reported globally.1 2
Risk factors for developing pituitary abscesses include structural disorders such as pre-existing pituitary lesions such as craniopharyngioma, pituitary adenoma and Rathke’s cleft cyst, as well as historical features such as immunosuppression, prior surgical intervention in the sella or irradiation to that area.3 4 The most common risk factor reported was history of pituitary surgery, present in 38.5%–41.7% of cases. However, 70% of cases occur de novo in a normal pituitary gland.2–8 Abscesses can arise either by haematogenous seeding of the pituitary gland or by extension from an adjacent infection, such as meningitis, sphenoid sinusitis, thrombophlebitis or contaminated cerebrospinal fluid (CSF) fistula.4 6 7 Causative organisms described in causing pituitary abscesses represent a wide spectrum of pathogens. Most common are gram-positive cocci (50%); other agents are gram-negative bacilli and in immunocompromised individuals, fungi such as yeast, aspergillus and histoplasma have been reported. In up to 60% of cases, no pathogen could be identified, which can occur if there is preoperative antibiotic therapy or inadequate collection technique.2–8 In our case, the patient had a known history of a pituitary lesion, which is a risk factor for developing abscess. In this patient, the culture grew S. epidermidis, although there was concern for potential uncultured organisms.
Preoperative diagnosis can be challenging, both because of the rarity of the disease and the non-specific symptoms. In our patient, an abscess was not suspected given her lack of fever, leucocytosis or meningeal symptoms. However, fever has only been reported in 13%–57% of cases and meningismus symptoms reported in 16%–57%. The most common presenting complaint was headache (69%–100%), followed by anterior pituitary dysfunction (54%–84%) and visual disturbances (27.3%–100%).2–8 Unfortunately, these symptoms are non-specific for pituitary abscess and can be seen with pituitary lesions. Diabetes insipidus is reported in 41%–70% of cases, which is a less common endocrinopathy to occur preoperatively.3 6 7 If there is concern, a patient has developed a pituitary abscess, specific questions regarding polyuria, polydipsia or nocturia may help narrow the differential. There has been consideration to classify abscesses into acute, subacute and chronic categories finding infectious symptoms more common in the acute and subacute categories and lacking in the chronic category.3 6 7
Preoperative imaging is an effective way of characterising pituitary lesions. Computer tomography, though not the preferred imaging modality to characterise pituitary lesions, typically shows erosion and enlargement of the sella turcica and in some cases a well-defined low-attenuation rounded lesion with ring enhancement. The preferred imaging modality is MRI. Typical features include cystic lesions with isointensity or hypointensity on T1-weighted and isointensity or hyperintensity on T2-weighted imaging. Peripheral rim enhancement can be appreciated after gadolinium contrast. The proper clinical context should be applied, as similar characteristics can be seen with other sellar lesions, such as craniopharyngiomas and Rathke’s cleft cysts.1–8 Assessing the apparent diffusion coefficient on imaging might be helpful, as abscesses will have a reduction in the apparent diffusion coefficient, whereas necrotic tumours will have higher values.9
The mainstay of therapy is trans-sphenoidal surgical excision, followed by antibiotic therapy for 4–6 weeks. Empiric therapy consists of ceftriaxone and metronidazole infusions with vancomycin if concerns for Staphylococcus aureus are present prior to culture data guiding therapy.2–6 In our case, the patient was initially started on ceftriaxone and vancomycin before transitioning to daptomycin and ertapenem after consultation with infectious disease.
Due to improvements in therapy for pituitary abscesses, mortality has declined from 45% to 10%.5 7 At follow-up, >90% of patients report improvement in headaches, with 75% having improvement in visual symptoms versus 16% without change. Pituitary hormone recovery depends on whether the abscess occurred de novo or in a patient with secondary features, such as an underlying abscess, and when the deficiency began in association with when they developed the abscess. In new hormone deficiencies occurring with the abscess, 25% of patients had improvement in the deficiency and 63% had no change. Whereas, in patients where the deficiency had been present prior to developing the abscess, none of those patients had recovery of their hormone deficiency.4–8 In our patient, following surgery and antibiotic therapy, her new onset secondary adrenal insufficiency, which presumably started within the last 6 months coinciding with worsening of her chronic headaches and new weight loss, resolved. However, her pre-existing secondary hypothyroidism and amenorrhea diagnosed 3 years prior to presentation persisted.
Fortunately, recurrence rate for patients is low at ~13%, occurring more often in immunocompromised patients.3
Outcome and follow-up
Pituitary abscesses are a rare infection. This case highlights the importance of recognising a pituitary abscess even in a patient without meningeal signs. The patient is doing well at her 6-month and 12-month follow-up visits without new headaches or other symptoms.
Discussion
Pituitary abscesses are a rare infectious process in the sella. It is difficult to diagnose preoperatively due to its non-specific symptoms compared with other pituitary lesions. However, careful history particularly focusing on patient’s surgical history and symptoms of diabetes insipidus can help narrow diagnosis. Additionally, contrary to popular belief the most common symptoms are headache, pituitary hormone deficiency and visual disturbances with fever and meningismus rarely occurring. Management with surgical excision and antibiotics are the mainstays of therapy with a good recovery rate of constitutional symptoms, such as headache and visual disturbances but rare recovery rates of the hormone deficiencies. A summary of this information can be found in table 2.
Summary of pituitary abscess management
Learning points
Headache, anterior pituitary insufficiency and visual field deficits are the most common presenting symptoms of pituitary abscess.
Treatment consistent of surgical drainage of abscess, followed by antibiotics.
Normalisation of recent-onset pituitary hormone insufficiency may occur after surgery, but not long-standing ones.
Ethics statements
Patient consent for publication
Ethics approval
The manuscript has been approved by the ethical and IRB.
Acknowledgments
None.
Footnotes
Twitter @tdhdthanh
Contributors ZWB—author. TSK—reviewer and editor. ZSR—pathology resident reviewed and provided histopathology pictures. TDH—reviewer, editor and mentor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.