Article Text

Abstract
External-beam radiation therapy (EBRT) for differentiated thyroid cancer has been controversial. Palliative irradiation is usually recommended for patients with treatment-resistant relapse and/or distant metastases, but high-dose EBRT is not often indicated in this situation. A 50-year-old man had treatment-resistant recurrence of an inoperable cervical mass and multiple lung metastases after total thyroidectomy and neck dissection. Because the patient had good performance status and no other life-threatening metastases, he received high-dose intensity-modulated radiation therapy (IMRT). Remarkably, the tumour shrank during treatment. After 3 months, he had bleeding from the internal carotid artery. The bleeding was outside the high-dose irradiation site and was likely due to infection; emergency interventional radiology was performed. The post-EBRT clinical course was favourable and the cervical mass almost disappeared. The patient remained alive for 3 years post treatment. It is possible to extend the indication of high-dose intensity-IMRT in selected patients with differentiated thyroid cancer.
- head and neck cancer
- radiotherapy
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Differentiated thyroid cancers (DTC), which encompass papillary, follicular and mixed papillary–follicular histologies, account for approximately 90% of thyroid cancers; standard treatments are surgery, radioactive iodine treatment, thyroid-stimulating hormone-suppressive therapy and molecular-target drug treatments.1 The prognosis of DTC is better than that of other carcinomas because of its slow progression and long-term survival may be expected even if distant metastasis is observed. Even in cases with metastases to the lung (the most frequent metastatic site), the survival rate of 131I-avid patients was 87.0% at 5 years and 69.2% at 10 years and the survival rate of non-131I-avid patients was 69.7% at 5 years and 38.1% at 10 years.2
Following good locoregional control of the primary DTC lesion by radical external-beam radiation therapy (EBRT), the American Thyroid Association Management Guidelines recommend surgery combined with radioactive iodine and/or EBRT for postoperative cases which have residual lesions and high-risk recurrence factors or for cases in which tumours invade the upper aerodigestive tract.3–5 However, there are reports denying the benefit of additional EBRT, and the role of EBRT for DTC has been controversial.6–8 Intensity-modulated radiation therapy (IMRT) makes it possible to increase the irradiation dose to tumours by reducing the organ-at-risk (OAR) dose and it is expected that the indications for EBRT will be expanded in the future.1 4 9
In cases of recurrence and metastasis in DTC, palliative EBRT for treatment-resistant bone metastasis, brain metastasis and lung metastasis is useful for symptom relief. Moreover, even in selected cases with distant metastases, EBRT may prolong survival.10 The National Comprehensive Cancer Network Guidelines recommend considering higher-dose irradiation (45–60 Gy) in 1.8–2 Gy daily fractions or stereotactic body radiation therapy for patients with oligometastatic disease and good performance status.11 However, the optimal dose and patient selection in such cases have not been established. Additionally, high-dose EBRT carries risks such as radiation pneumonitis, esophagitis, tracheitis and arterial perforation.12 We report a case of inoperable recurrent papillary thyroid cancer presenting with an inoperable cervical mass and multiple lung metastases successfully treated with high-dose IMRT.
Case presentation
A 50-year-old man with no previous history of illness was diagnosed with stage I papillary thyroid cancer, tall-cell variant and underwent total thyroidectomy. Two years later, he developed lymph-node and multiple lung metastases and underwent additional neck dissection and radioactive iodine treatment, thyroid-stimulating hormone-suppressive therapy and sorafenib and lenvatinib therapies; unfortunately, he developed resistance to these therapies. Seven years later, the cervical tumour was observed during regular follow-up to have gradually increased in size and additional neck dissection was scheduled. However, the lesion was judged to be inoperable because of its rapid growth just before surgery and radiation therapy began 1 week later. At the first visit to our department, the patient’s left cervical lymph-node metastasis had markedly increased to 13 cm maximum diameter and the tumour had grown circumferentially around the common carotid artery (CA). The patient was referred to our department for palliative EBRT to reduce exudates and bleeding.
CT scan showed lymph-node metastases not only in the left neck but also in the axilla and mediastinum, which squeezed the superior vena cava (figure 1). Many small lung metastases were also observed. The patient had good performance status, had no dysphagia that could lead to aspiration pneumonia, had no complications that increased the risk of adverse event from high-dose irradiation and had no other life-threatening distant metastatic lesions; therefore, we presented high-dose IMRT as an alternative to standard palliative irradiation. Although this case presented with a huge cervical mass, fiber–optic investigation of the pharynx showed no airway narrowing and no symptoms of facial oedema, suggesting that emergency irradiation was not indicated. That is, 1 week of IMRT treatment was considered acceptable. The purpose of this treatment was to prevent fatal airway obstruction and to prolong patient survival by maintaining tumour shrinkage from the high-dose irradiation, in addition to alleviating symptoms such as exudates and bleeding. The patient understood the risks of mucositis, oesophageal stricture and perforation, pneumonitis and arterial bleeding due to high-dose EBRT and consented to the treatment. During EBRT, he received no systemic treatment.

Pretreatment images: body-surface image (A) and enhanced CT scan in coronal plane (B). Images 1 year after treatment: body-surface image (C) and enhanced CT scan in coronal plane (D).
Treatment
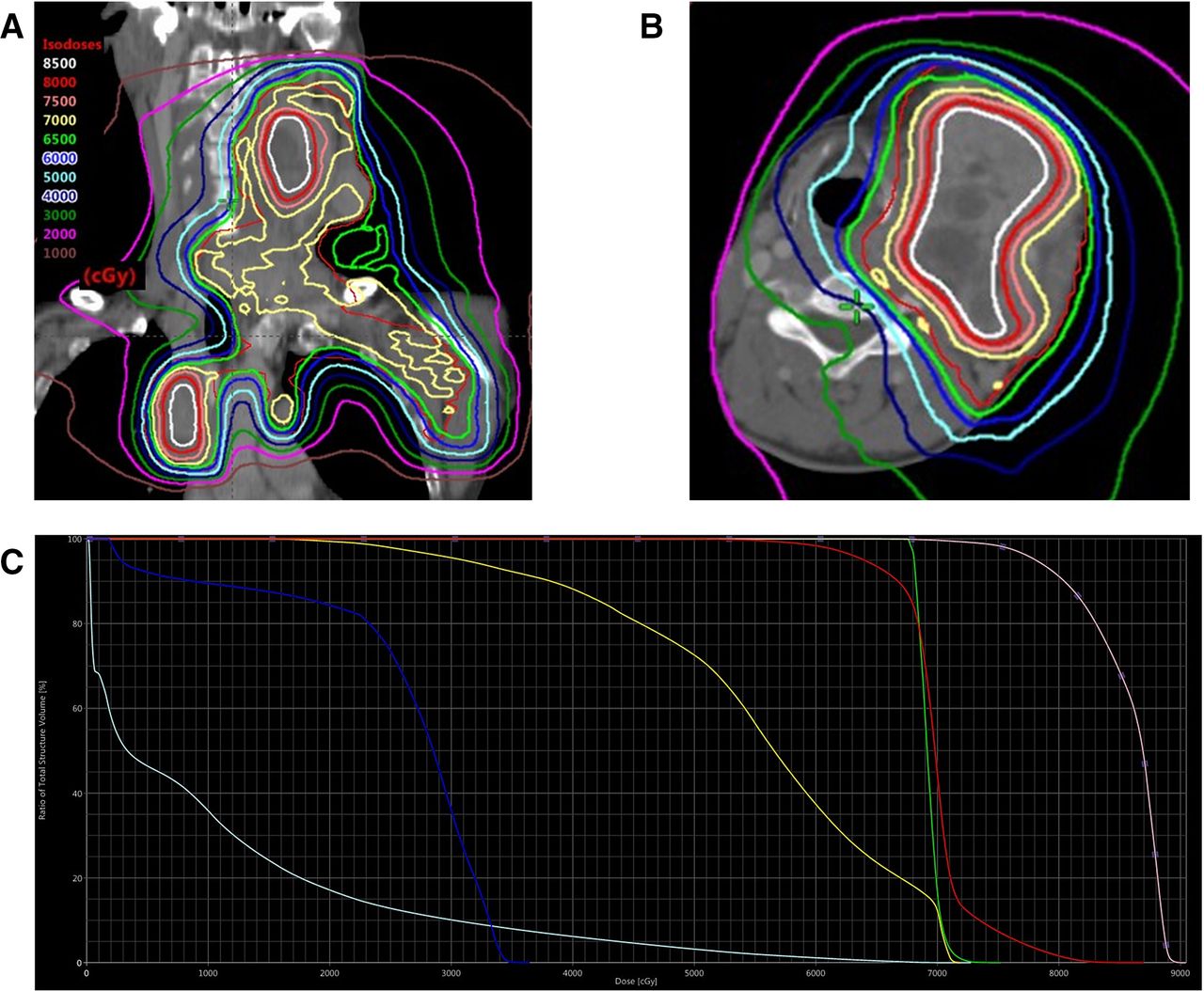
A series of metastatic lymph nodes, extending from the left neck to the axilla and mediastinum, was set as the gross tumour volume (GTV). Planning target volume (PTV) margins of 5 mm were added to the GTV to cover set-up error. We provided IMRT with 6 MV photons produced by a TomoTherapy HD system (Accuray, Sunnyvale, CA). IMRT was performed for a total of 35 fractions over 7 weeks using the simultaneous integrated boost (SIB) and simultaneous integrated protection (SIP) methods. The central GTV dose was over 2.5 Gy/fraction and the marginal dose for PTV was 2 Gy/fraction to reduce the OAR dose (figure 2). The maximum dose at the CA was 75.3 Gy by IMRT. To respond to dosimetric changes due to tumour and body-shape shrinkage during IMRT, the replanning CT scan was performed twice during treatment and the treatment plan was changed at 15 fractions and 30 fractions. The patient completed all IMRTs without severe acute adverse effects during treatment.

{kind=link}
{kind=link}
Dose distribution of intensity-modulated radiation therapy in coronal plane (A) and axial views at laryngeal (B). (C) Dose volume histogram depicting the dosimetric parameters analysed at the central gross tumour volume (pink), marginal planning target volume (red), left carotid artery (green), trachea (yellow), spinal cord (blue) and lungs (light blue).
Outcome and follow-up
The neck mass shrank remarkably and the exudate decreased. After 3 months, the patient exhibited bleeding from the left internal CA and underwent emergency interventional radiology. At the immediately previous examination, blood sampling had shown an increased white blood cell count of 10.4×109 cells/L and C reactive protein of 10.9 mg/L and there had been pus outflow and swelling from the affected area, suggesting infection. In addition, CT scan also showed air, suggestive of infection around the left internal CA. The left common and left internal CAs were embolised with coils; the patient survived without neurological symptoms. The postradiation therapy clinical course was favourable and the left cervical mass almost disappeared 1 year after treatment (figure 1). After radiation therapy, resumption of systemic treatment was considered, but it was not resumed in accordance with the patient’s wishes. Regular follow-up 1 year and 8 months after radiation therapy revealed a regrowth of the left neck mass and an increase in multiple lung metastases; low-dose lenvatinib (4 mg/day) administration was resumed.
Tumour growth slowed without major adverse events after resumption of lenvatinib. The patient remained alive for 3 years after radiation therapy.
Discussion
High-dose EBRT and stereotactic body radiation therapy for DTC are associated with a high local-control rate and may prolong survival in selected patients, even with recurrent lesions or metastases.13 14 Randomised trials of patients with distant metastases of prostate cancer showed that additional radiation therapy to the primary lesion resulted in better overall survival and failure-free survival in patients with low metastatic burden.15 However, patient selection in such cases with DTC has not been established. Brierley and Sherman advocated that patients with uncontrolled cervical lesions are good candidates for high-dose radiation therapy because these patients may survive longer, despite metastatic DTC.10 In DTC cases with lung metastases, age (<40 years), the presence of multiple distant metastases (excluding lung and lymph-node metastasis) and pulmonary metastatic node size (<1 cm) have been reported as independent prognostic factors regardless of iodine accumulation.2 Our case is a tall-cell variant of papillary thyroid cancer, which has clinical features such as more invasive and advanced staged cases, higher recurrence rate and higher mortality rate than conventional papillary thyroid cancer.16 Actually, he had multiple small (<1 cm) lung metastases and no other distant metastases. Excluding cervical lymph-node metastases, the prognosis for iodine-refractory multiple lung metastases was expected to be 70% in 5 years.2 Therefore, we aimed to control the cervical lesions while reducing the risk of adverse events by using high-dose IMRT. Because the patient’s lesions were huge and surrounded the CA, the dose to the tumour should have been increased, but there was a risk of arterial bleeding. Therefore, we treated him with IMRT using the SIB and SIP methods, which can increase the central dose of a tumour while controlling the OAR dose around the tumour.17 High-dose irradiation with this method increased local control and overall survival for unresectable intraductal cholangiocarcinoma lesions.18 Although DTC is generally considered to be radiation resistant, there are reports of good local control by high-dose irradiation. Irradiation of 50 Gy or more for DTC with curative intent gives good local control; the 5-year local recurrence rate was reported as 15%.13 Similarly, a high local-control rate has also been reported for stereotactic body radiation therapy for metastatic lung tumours, including DTC.14 In our patient, huge cervical lymph-node, mediastinum and axilla metastases were almost eliminated without any acute adverse events such as mucositis or pneumonitis. After 3 months, he exhibited bleeding from the left internal CA, from 2 cm cranial to the bifurcation of the internal CA and from outside the high-dose irradiation range (<70 Gy). The bleeding was probably caused by infection, but we could not completely rule out high-dose irradiation as a cause of the bleeding. High-dose irradiation, such as reirradiation, can also cause arterial bleeding in patients with head and neck cancer. Other risk factors for arterial bleeding are tumour invasion of more than half of the CA, ulceration, necrosis and large single-fraction dose.19–21 Because the risk of arterial bleeding was originally considered to be very high in this case, the single-fraction dose was small and the CA dose was reduced by IMRT. During treatment, care such as daily cleaning and application of protective agents was performed by medical staff, but lack of self-care guidance after treatment might increase the risk of bleeding due to infection.
Application of high-dose EBRT for DTC will be expanded by using IMRT technology, even for metastatic and recurrent cases.10 It was considered to be particularly useful for patients with oligometastases and good performance status.11 IMRT treatment requires considerable human and time resources, so it is not justified in all cases with multiple metastases. Because DTC generally progresses slowly and a relatively long-term prognosis can be expected in selected cases, appropriate case selection should be considered in the future even in cases of multiple distant metastases. High-dose irradiation of large lesions involves the risk of arterial bleeding and it is necessary to continue to study optimal case selection, irradiation dose levels and treatment management.
Learning points
Application of external-beam radiotherapy (EBRT) for differentiated thyroid cancers (DTC) will be expanded by using intensity-modulated radiation therapy technology.
High-dose EBRT for DTC is associated with a high local-control rate and may prolong survival in selected cases, especially those with metastatic or refractory cervical lesions as oligometastases and good performance status.
Risk factors for arterial bleeding by EBRT are tumour invasion of more than half of the carotid artery, ulceration, necrosis and large single-fraction dose.
Ethics statements
Patient consent for publication
Acknowledgments
The authors thank Edanz (https://jp.edanz.com/ac) for editing a draft of this manuscript.
References
Footnotes
Contributors YK was involved in patient management, manuscript writing and image acquisition. SO was involved in patient management and manuscript writing. FM and KS were involved in clinical oversight and manuscript review. All authors reviewed and approved the final version of the article before submission.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.