Article Text

Statistics from Altmetric.com
Description
A 63-year-old Japanese woman presented with a 9-month history of productive cough. Although she had been treated with oral antibiotics (amoxicillin and levofloxacin), her symptoms worsened. She had no history of allergic diseases, including asthma, except for known allergies to eggs. She had never smoked.
Her vital signs and physical examination were unremarkable. Laboratory tests revealed white blood cell count of 12.26×109/L (normal: 3.3–8.6×109/L) with absolute eosinophil count of 2.45×109/L (normal: 0.10–0.30×109/L), serum total IgE levels of 235 IU/mL (normal:<173 IU/mL), Aspergillus-specific IgE levels of 5.49 UA/mL (normal: <0.35 UA/mL), positive for Aspergillus-specific precipitin and negative for serum antigen of Aspergillus spp.
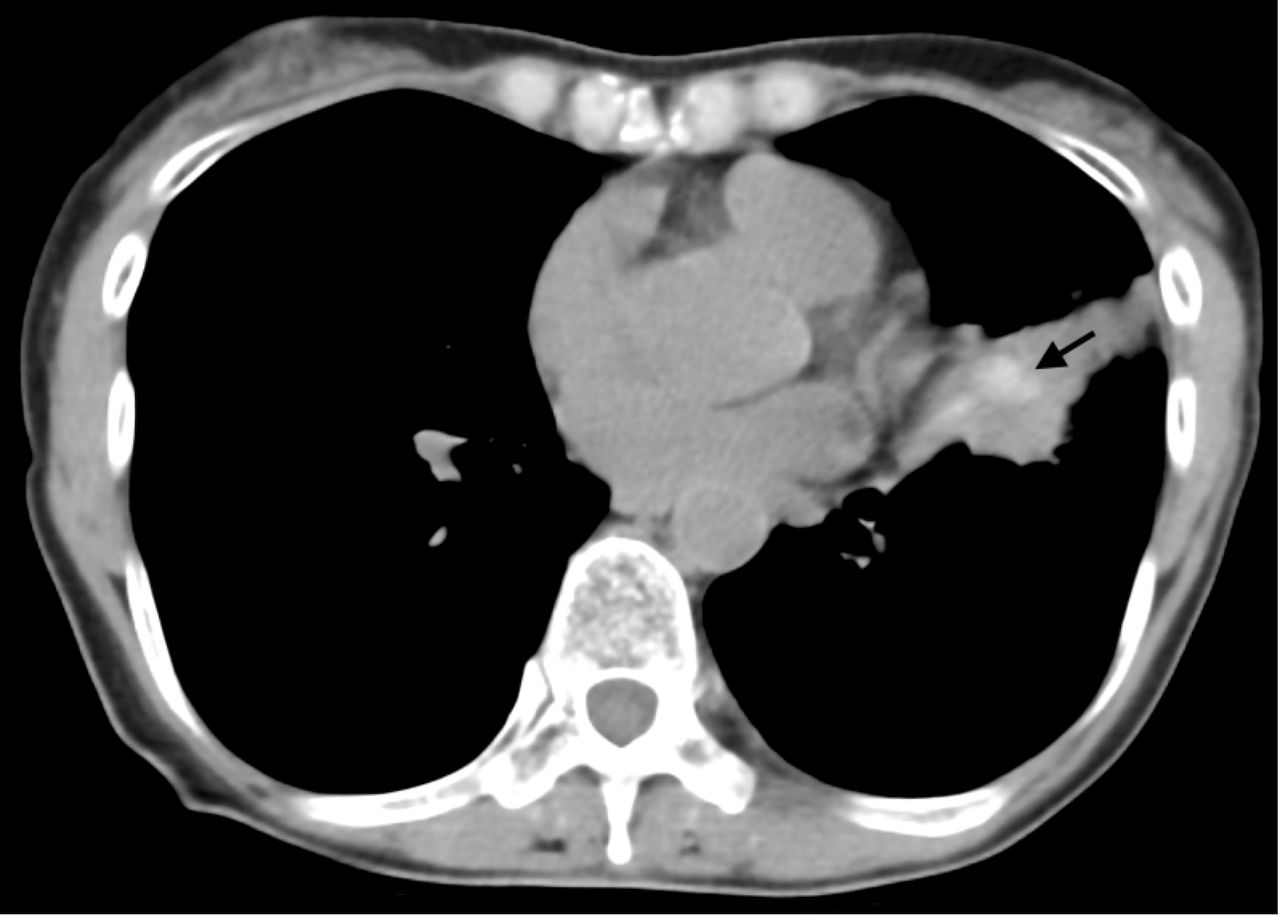
Chest radiography showed consolidation in the left middle lung field. Chest CT revealed high-attenuation mucus (HAM), a typical finding in allergic bronchopulmonary aspergillosis (ABPA), and central bronchiectasis (figure 1). We performed a transbronchial biopsy of the mucus plugs in the left upper lobe. Pathological findings showed remarkable eosinophil infiltration with Charcot-Leyden crystals, and branching hyphae on Grocott stain (figure 2). In the culture of bronchial lavage fluid, Aspergillus fumigatus was detected.

Chest CT shows high-attenuation mucus (arrow).

{kind=link}
{kind=link}
Grocott stain for biopsied specimen of mucus plugs shows branching hyphae (arrows).
Consequently, the patient fulfilled 8 of 10 components in the criteria for allergic bronchopulmonary mycosis (ABPM) by the Japan ABPM Research Programme.1 Therefore, we confirmed the diagnosis of ABPA, and subsequently, prednisolone with tapering was administered. After the treatment, her symptoms, eosinophilia and consolidation on chest radiography were gradually improved.
ABPM is a disease caused by an allergic reaction to fungi in the lower respiratory tract, especially those caused by Aspergillus spp are called ABPA.2 There are several clinical diagnostic criteria for ABPM, including Rosenberg-Patterson criteria proposed in 1977,3 the International Society for Human and Animal Mycology (ISHAM) criteria in 20134 and the Japan ABPM Research Programme criteria in 2020.1
The Rosenberg-Patterson criteria have a high specificity of 98.4% but a low sensitivity of 49.2%, while the ISHAM criteria have a sensitivity of 82.7% and a specificity of 86.8%. In contrast, the sensitivity and specificity of the Japan ABPM Research Programme criteria are 94.4% and 90.0%, respectively, indicating that ABPM can be diagnosed with high accuracy.1
ABPM often shows mucoid impaction, and its differential diagnosis includes endobronchial lesions or foreign bodies, bronchial atresia and bronchiectasis due to various causes.5 HAM is defined as mucus plugs with higher densities than paravertebral muscles on high-resolution CT, and the CT density value of 70 Hounsfield units is an adequate cut-off value.6 It has been assumed that iron, manganese and calcium produced by fungi in the mucus may cause higher densities.6 The sensitivity and specificity of HAM for ABPA are reported as 39.7% and 100%, respectively.7 HAM is an important finding in the early diagnosis of ABPM.
Learning points
Allergic bronchopulmonary mycosis can be diagnosed by Japan Allergic Bronchopulmonary Mycosis Research Programme criteria with higher accuracy than other criteria.
High-attenuation mucus is an important finding in the early diagnosis of allergic bronchopulmonary mycosis.
Ethics statements
Patient consent for publication
Acknowledgments
We thank Editage (www.editage.com) for English language editing.
Footnotes
Contributors SI and HS drafted the manuscript. TT and KN revised the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.