Article Text

Abstract
Cerebral venous sinus thrombosis (CVST) following novel coronavirus-2019 (nCoV-19) vaccination is a rare adverse effect. We report the first case of CVST associated with ChAdOx1 vaccination, with positive anti-platelet factor 4 (PF4) antibodies, from India. A 44-year-old woman developed a thunderclap headache 4 days after the first dose of the adenoviral vector vaccine ChAdOx1 (Covishield). Physical examination was unremarkable barring mild neck stiffness with no focal neurological deficits. MRI identified right transverse sinus thrombosis. Laboratory tests revealed raised D-dimer and thrombocytopenia; anti-PF4 antibodies were subsequently identified, consistent with thrombosis with thrombocytopenia syndrome (TTS). She was treated with non-heparin anticoagulation and intravenous immunoglobulin and made an uneventful recovery. Early recognition of adenoviral vector vaccine-related TTS, which resembles heparin-induced thrombocytopenia syndrome, is important as heparin and heparin analogues are best avoided in the treatment.
- COVID-19
- immunological products and vaccines
- global health
- vaccination/immunisation
- neuroimaging
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
Background
As of 22 August 2021, more than 446 million doses of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) vaccines have been administered in India; 127 million people have been fully vaccinated (9.3%) and 319 million have been given at least one dose; of these, more than 90% have been administered the ChAdOx1 (Covishield) vaccine. Only rare serious neurological adverse events following immunisation such as Guillain-Barré syndrome have been reported following the ChAdOx1 vaccine in India.1 Recently, an immune thrombocytopenic disorder associated with cerebral venous sinus thrombosis (CVST) has been described following replication-deficient adenoviral vector vaccines such as the Chimpanzee adenovirus-based ChAdOx1 (Oxford/AstraZeneca) and the Human adenovirus-based Ad26.COV2.S (Janssen/Johnson & Johnson) vaccines.2 3 Initially, it was termed vaccine-induced prothrombotic immune thrombocytopenia syndrome or vaccine-induced thrombotic thrombocytopenia. Now it has been renamed thrombosis with thrombocytopenia syndrome (TTS). We report the first case of definite TTS with CVST and positive anti-platelet factor 4 (PF4) antibodies from India.
Case presentation
A 44-year-old woman developed a thunderclap headache at 2:00, which woke her up from her sleep. Four days before her headache, she had received her first dose of ChAdOx1/Vaxzevria (Covishield; Serum Institute of India, Pune, India) vaccination. As the headache persisted for 2 days, she presented to hospital. On examination, she had mild neck stiffness and papilloedema bilaterally without any other focal deficits.
Investigations
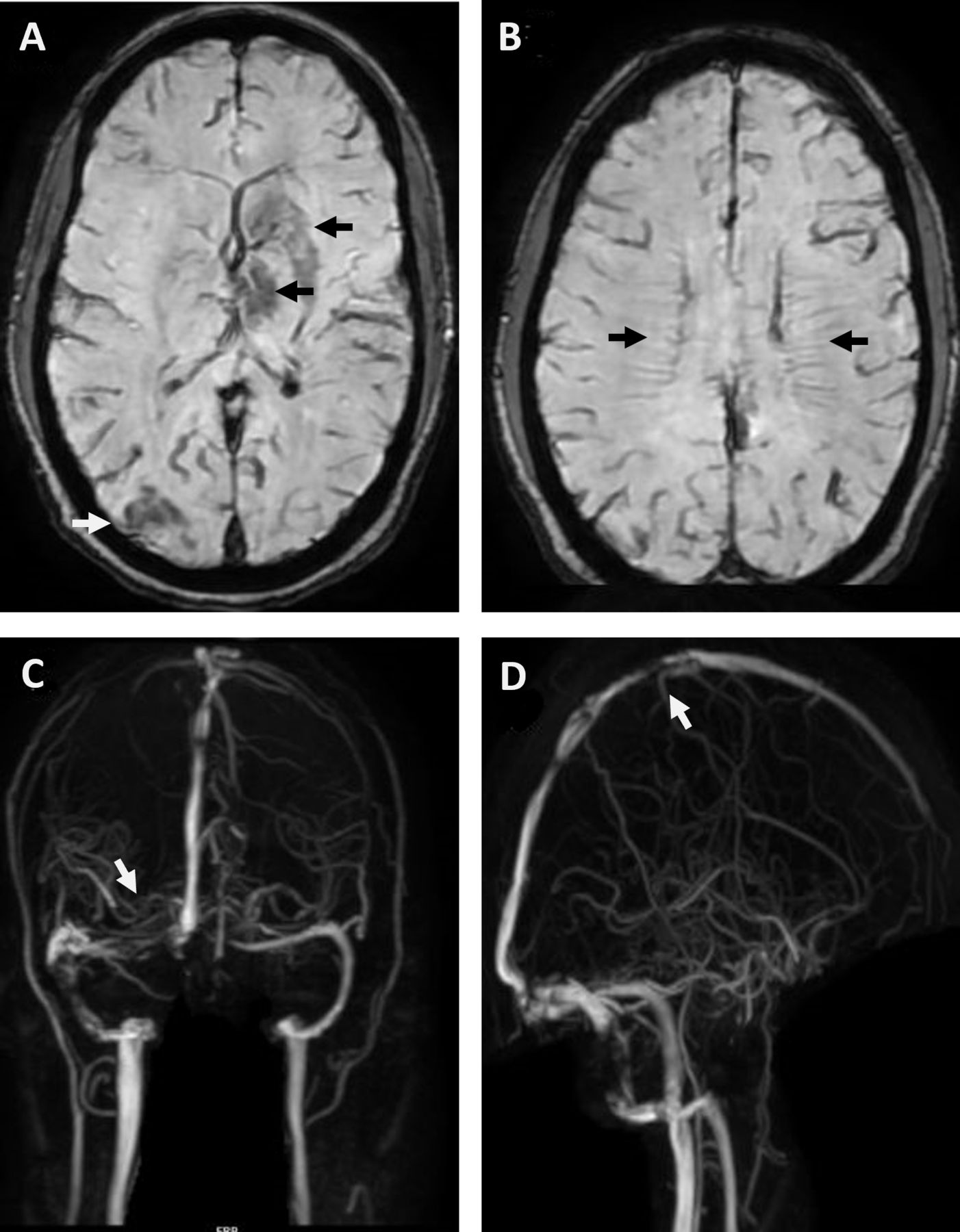
Magnetic resonance (MR) brain scan with fluid attenuated inversion recovery sequences showed high parietal sulcal hyperintensities suggestive of sulcal subarachnoid haemorrhage; MR gradient echo sequences showed haemorrhagic infarcts (figure 1A) and venous congestion in the medullary veins (figure 1B). MR venogram showed poor flow in the posterior portion of the superior sagittal sinus and right transverse sinus thrombosis (figure 1C,D). Laboratory tests showed thrombocytopenia (80 000 /µL; normal 150 000–400 000 /µL) and elevated D-dimer (>20 000 ng/mL; normal <500 ng/mL). Reverse transcriptase PCR test for SARS-CoV-2 on a nasopharyngeal swab was negative. Serum lactate dehydrogenase was normal and peripheral smear did not show any schistocytes. A prothrombotic workup (serum Homocysteine, Factor V Leiden, Protein C, Protein S, methylenetetrahydrofolate reductase (MTHFR) mutation and Prothrombin gene 20 210 mutations) was negative. While anti-PF4 antibodies were not detected by the locally available particle gel or chemoluminescent immunoassays, the ELISA test (Hyphen Biomed ZYMUTEST HIA IgG & IgGAM; Christian Medical College, Vellore, India) recommended by international guidelines was positive.

MRI brain scans. (A) Axial gradient echo image showing left basal ganglia and thalamic haemorrhagic infarctions (black arrows), and right occipital haemorrhagic infarction (white arrow). (B) Axial gradient echo image showing bilateral prominent congested medullary veins (black arrows). (C) Venogram image showing reduced flow in the right transverse sinus (white arrow). (D) Venogram image showing reduced flow in the posterior superior sagittal sinus (white arrow).
Differential diagnosis
The differential diagnosis of TTS, thrombotic thrombocytopenic purpura (TTP), microangiopathic hemolytic anaemia (MAHA) and other prothrombotic conditions were considered. Due to the combination of thrombocytopenia, high D-dimer, CVST, temporal relationship to ChAdOx1 vaccination and the absence of features of MAHA (characterised by the constellation of thrombocytopenia, anaemia and red blood cell fragmentation (schistocytes) on the blood film), TTS was considered most likely.
Treatment
She had been started on low molecular weight heparin (LMWH) for 1 day at another centre prior to transfer to our centre. LMWH was discontinued and she was started on mannitol, levetiracetam and fondaparinux with a diagnosis of probable TTS. On day 9, her headache worsened and she developed new purpuric spots on her right forearm. Her platelet counts dropped to 45 000/µL and her headache worsened. Intravenous immunoglobulin (IVIg) 2 g/kg by body weight was administered over 2 days and fondaparinux was continued. Over the next 4 days, her platelet counts improved to 200 000/µL and she improved symptomatically. She was started on oral dabigatran prior to discharge from hospital.
Outcome and follow-up
She has made a full recovery and remains asymptomatic on 6-week follow-up. She has been advised to continue oral dabigatran for 4–6 months, although there is no guideline at present regarding long-term anticoagulant or antiplatelet prophylaxis.
Discussion
As of 22 August 2021, more than 4.91 billion vaccine doses have been administered worldwide. TTS has been reported only with adenoviral vector vaccines and there are no reports with mRNA vaccines such as Pfizer/BioNTech or Moderna nCoV-19 vaccines. There seems to be a geographical difference in the reported incidence of TTS across the world as very few cases have been reported from non-European countries.4 Norway has reported a rate of 1 per 25 000 vaccine doses, Germany 1 per 100 000 doses, while Europe’s overall figure is 1 per 210 000 doses.4 In the UK, the reported incidence is 1 in 500 000 doses.4 Thus, the risk of developing TTS is very low overall. Most cases of TTS have been reported after the first dose of ChAdOx-1 vaccine. Although the risk is thought to be lower with the second dose, it has to be borne in mind that substantially fewer second doses of the ChAdOx-1 vaccine have been administered so far.4 Thrombosis often involves unusual sites such as the cerebral venous sinus or splanchnic circulations. However, other sites such as deep vein thrombosis, pulmonary thromboembolism, arterial strokes, myocardial infarction or multi-organ thrombosis can occur.
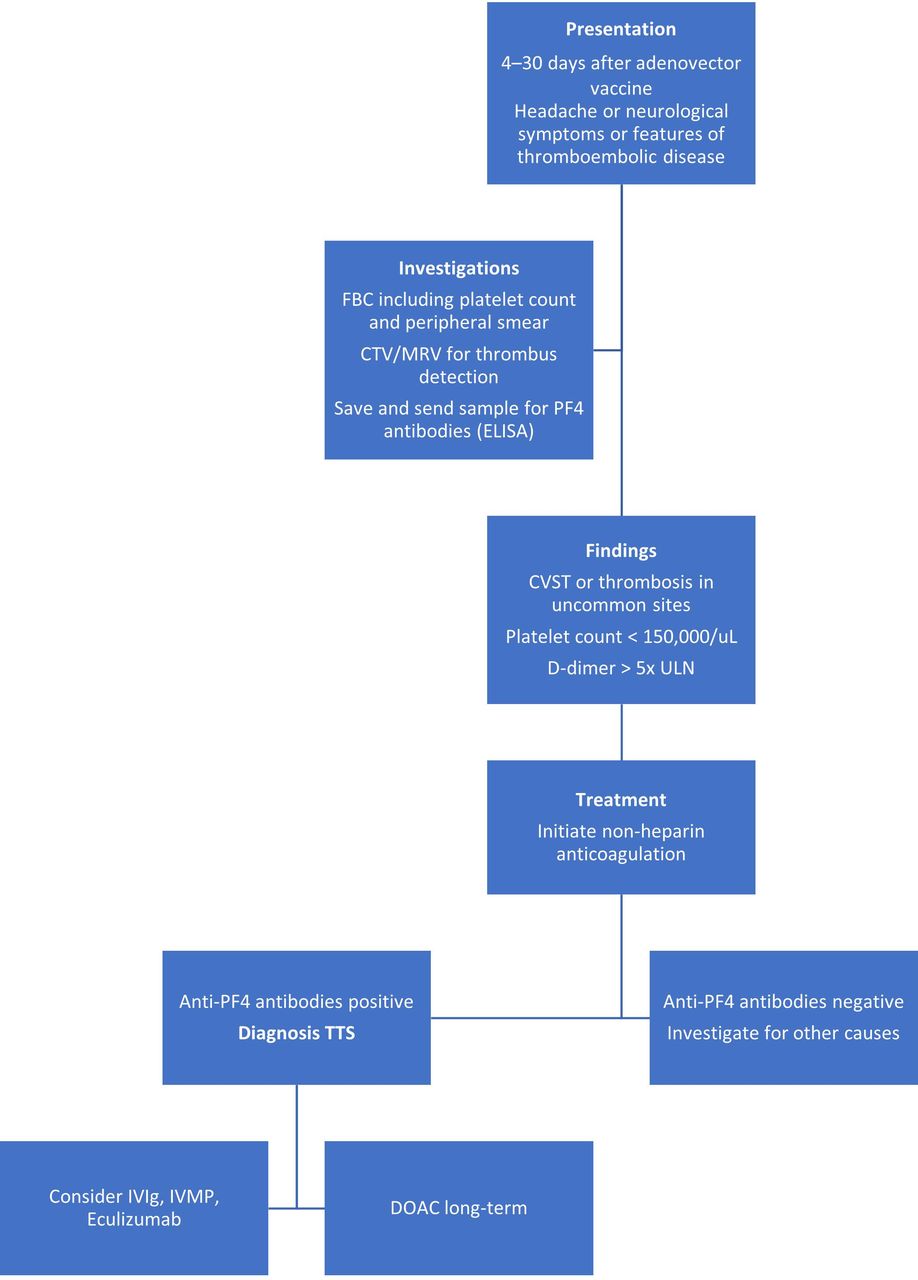
Most of the patients who develop TTS are younger than 50 years, female (75%), and do not have pre-existing pro-thrombotic risk factors or a history of heparin administration. TTS often occurs within 4–30 days after vaccination and an algorithmic approach is useful (figure 2). With early diagnosis, morbidity and mortality can be reduced. The American Society of Haematology5 has laid down the following diagnostic criteria for TTS (all four criteria must be fulfilled for definite TTS):
A history of adenoviral vector vaccination 4–30 days before the onset of thrombosis.
Venous or arterial thrombosis (involving the cerebral or abdominal vasculature predominantly such as CVST or splanchnic thrombosis).
Thrombocytopenia (<150 000/µL).
Positive anti-PF4 antibodies by ELISA testing.
{kind=link}
{kind=link}
Algorithm for diagnosis and treatment of thrombosis with thrombocytopenia (TTS) syndrome.4–6 CTV, computed tomographic venogram; CVST, cerebral venous sinus thrombosis; DOAC, direct oral anticoagulant; FBC, full blood count; IVIg, intravenous immunoglobulin; IVMP, intravenous methylprednisolone; MRV, magnetic resonance venogram; PF4, platelet factor 4; ULN, upper limit of normal.
The particle gel immunoassay and chemiluminescent immunoassay tests for anti-PF4 antibodies, which are commonly performed in India, are not reliable in TTS. Platelet functional assays (serotonin release assay) have high sensitivity (>95%) and specificity (>95%) but are not widely available. Furthermore, anti-PF4 antibody tests may not be easily available in resource-poor or remote settings.
The WHO4 classification of TTS following vaccination with a COVID-19 vaccine includes three mandatory criteria:
Vaccination against COVID-19 within the last 30 days.
No alternative explanation for the condition (ie, no heparin exposure within the previous 100 days).
Combination of thrombosis and thrombocytopenia (<1 50 000/µL or <50% of baseline platelet counts).
The mechanism of TTS is similar to heparin-induced thrombocytopenia (HIT). In both conditions, IgG antibodies recognise PF4 bound to platelets and cause platelet activation, platelet consumption, hypercoagulability and thromboembolic complications. Unlike HIT, the IgG antibodies in TTS are produced without any prior exposure to heparin and are triggered by vaccine components.
Crucially, treatment options differ from the conventional treatment of CVST. Heparin and LMWH are best avoided if TTS is suspected. Instead, non-heparin anticoagulants should be used until TTS is conclusively ruled out. Alternatives include parenteral direct thrombin inhibitors (argatroban or bivalrudin, provided the baseline aPTT is normal), fondaparinux, danaparoid or direct oral anticoagulants. IVIg 1 g/kg by body weight daily for 2 days is recommended in unwell patients.4 As TTS can progress even after IVIg, patients need to be monitored and started on anticoagulation as early as possible. Anticoagulants should be continued even if bleeding complications occur (as long as the platelet counts are greater than 20 000 /µL or increasing after IVIg). Fibrinogen replacement can be considered in such circumstances. Platelet transfusions should be avoided in this consumptive coagulopathy or administered only if patients develop severe thrombocytopenia, life-threatening bleeding or require emergency surgery. Corticosteroids are sometimes used with IVIg although there are no guidelines regarding this combination. Plasma exchange can be used in treatment resistant cases, as also complement inhibitors such as eculizumab.6
At present, it is not known how long anti-PF4 antibodies in COVID-19 vaccine–related TTS persist. In patients with conventional HIT, immmunoassays can remain positive in 35% of patients for up to 1 year. Thus, there may be a risk for recurrent thrombosis because of circulating anti-PF4/heparin antibodies. It is important to advise patients who have completed only the first dose of ChAdOx1 vaccination to complete their vaccination schedule with an mRNA vaccine for the second dose.
To the best of our knowledge, this is the first case of definite TTS with anti-PF4 antibodies to be described from India. A case of CVST following ChAdOx1 vaccination without either thrombocytopenia or anti-PF4 antibodies has been described.7 However, this report did not fulfil the criteria for either definite or probable TTS and was probably a coincidental CVST. As adenoviral vector vaccines are the mainstay of COVID-19 vaccination programmes in India and most countries worldwide, prompt recognition and treatment of TTS by clinicians is vital for reducing mortality and morbidity from this rare but treatable condition globally.
Patient’s perspective
We were shocked to know that my mother had developed a blood clot in her head after COVID-19 vaccination. Around ten other people who had taken the same vaccine in our family did not have any problems after vaccination. My mother started complaining of headache which got worse very quickly. Although we met a couple of doctors, none of them were aware of such a complication. We are lucky that her condition was diagnosed early and that she got better with treatment. We only hope that our case helps other people with the same condition get diagnosed earlier and get better.
Learning points
Cerebral venous sinus thrombosis following adenoviral vector vaccines is a rare event.
It is associated with thrombocytopenia and anti-PF4 antibodies, and termed thrombosis with thrombocytopenia syndrome.
Unusual sites of thrombosis like the splanchnic, adrenal, cerebral and mesenteric veins can be involved.
Early recognition and treatment reduce mortality and morbidity.
Patients who have completed only the first dose of ChAdOx1 vaccination should complete their vaccination schedule with an mRNA vaccine for the second dose.
Ethics statements
Patient consent for publication
Footnotes
Contributors BVM and AAS designed the article. FMM and SV contributed to data acquisition and literature review. BVM wrote the first draft, which was revised and approved by all authors.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.