Article Text

Statistics from Altmetric.com
- ear
- nose and throat/otolaryngology
- medical management
- head and neck surgery
- otolaryngology / ENT
- plastic and reconstructive surgery
Description
A male inmate in his 20s presented to the otolaryngology clinic for evaluation of left ear swelling that began shortly after placement of gauge earrings in his bilateral ear lobes 2 years ago. About 1 month after insertion, his left ear became infected. He then tied two strings around the infected ear lobe in hopes that the ear lobe itself would subsequently detach. After each string was placed by the patient, two necrotic lobular keloid scars began to appear with surrounding purulent drainage, prompting him to seek medical attention. The patient reported minimal pain, and about 1 week of antibiotics was trialled without any improvement in his symptoms.
Physical examination showed a complex, pedunculated, bilobed keloid hanging from the inferior edge of the left auricular lobule (figure 1). Two separate lobulated masses were seen, tied off with the string at their base. There was partial necrosis of the inferior aspect, moderate purulent drainage, and the keloid was insensate (figure 2). The string foreign bodies were removed in clinic, and the decision was made to surgically excise the keloid mass with conscious sedation to maximise patient comfort and cosmetic outcome. The keloids were each grasped and cut from the lobule with curved iris scissors. Two distinct tissue defects remained on both the anterior and posterior aspects of the lobule. These were reapproximated with 5–0 fast absorbing gut suture, making sure not to overtighten suture and thus distort the integrity of the lobule. The patient was discharged with a 2-week course of ciprofloxacin. Unfortunately, the patient was not brought to his postoperative appointment, and he has been lost to follow-up since.

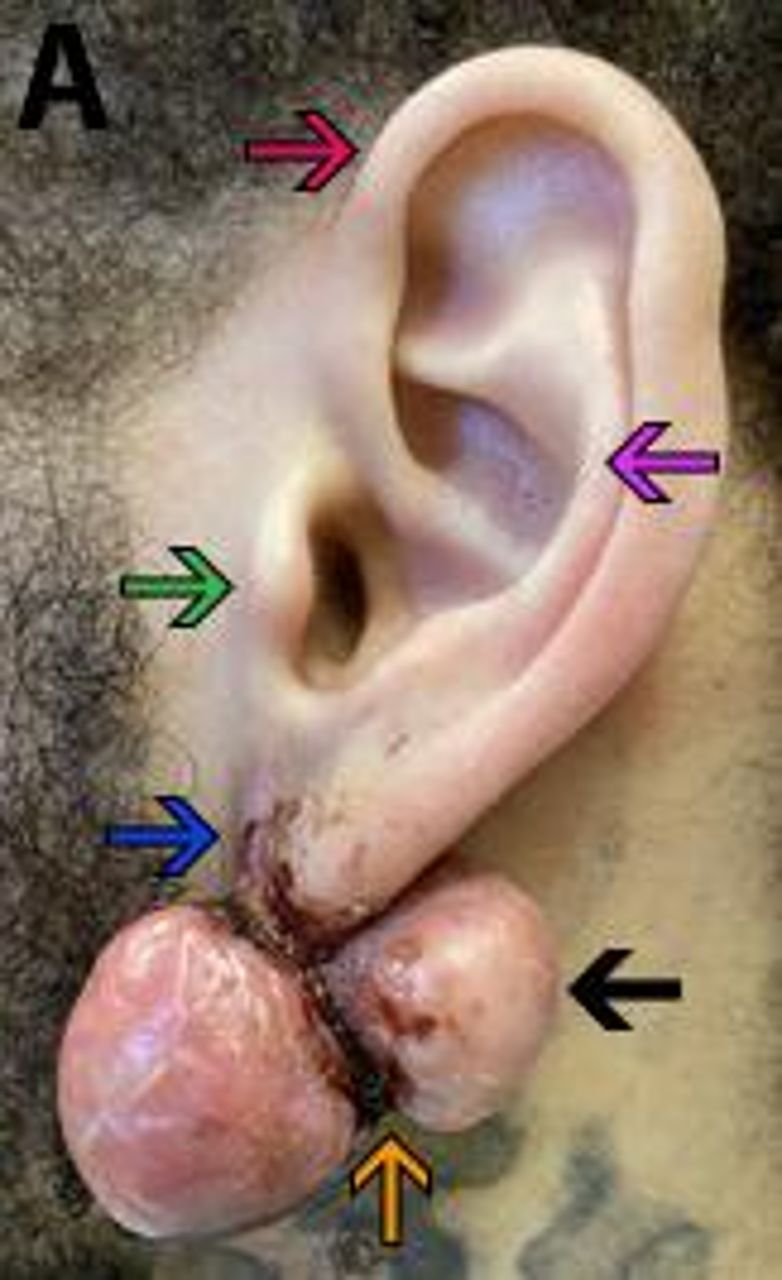
Lateral view of the multinodular sessile-type keloid scar (black arrow) of the pateint’s earlobe. Note the self-applied string (orange arrow) in an attempt to remove the keloid. Ear anatomy: helix (red arrow), antihelix (pink arrow), tragus (green arrow), lobule (blue arrow).

{kind=link}
{kind=link}
Inferior view of the patient’s multinodular sessile-type keloid scar (black arrows). Note the blackened, necrotic tissue at the inferior portion of the scar and the self-applied string (orange arrow). Ear anatomy: helix (red arrow).
Ear gauging begins similarly to the more common ear piercing with a 1 mm hole created in the auricular lobule, followed by expansion with increasing sizes of an ear plug.1 Keloids are the atypical proliferation of scar tissue at the location of cutaneous disruption and injury, characteristically growing beyond the original confines of the scar without regression. Keloid formation after earring placement may be predisposed by extrinsic trauma to the region, allergies to earring materials, infection due to non-sterile piercing conditions or otherwise, mechanical force from contact with a pillow during sleep, and the weight of the earring.2–5 It is unclear of the predisposing history in this patient’s case of keloid scarring; however, poor healthcare-literacy as evidenced by attempted self-amputation of the scar likely contributed to the extent of keloid formation and necrosis seen. Additionally, incarcerated and formerly incarcerated populations may present at later disease stages and often have lower levels of health literacy than the free world population.6
The patient’s multinodular sessile-type keloid was treated with radical keloidectomy, involving minimal amount of soft tissue to curtail further trauma. Closure of the injury along relaxed skin tension lines, skin grafts and targeting postoperative inflammation medically are common techniques used to minimise wound tension and reduce further scarring. Other treatment options may include occlusive dressings, radiation, laser therapy, cryotherapy and pharmacotherapy (eg, corticosteroids, 5-fluorouracil, imiquimod).7
Learning points
This patient’s keloid scarring was likely due to inflammatory complications of ear gauging, not uncommonly seen after placement of ear piercings or earrings.
Incarcerated populations have additional barriers to medical care compared with free world populations; these barriers should be taken into consideration when weighing appropriate treatment options.
Excision of the mass is a common treatment for keloid scarring, ideally involving minimal amounts of soft tissue and tension across the wound closure to reduce likelihood of keloid recurrence.
Ethics statements
Patient consent for publication
Footnotes
Contributors This manuscript is approved by all authors and has not been previously reported nor submitted for report in any other publication. Author contributions include drafting and editing of manuscript by DNR, NAR, JFO and OC. Concept, guidance and review of manuscript was completed by OC.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.