Article Text

Abstract
A 53-year-old non-smoking Japanese woman was admitted to our hospital with a 20-year history of wet cough and dyspnoea on exertion. Bronchial asthma (BA) had been diagnosed 20 years earlier. Although she has been treated with high-dose inhaled corticosteroid, she had experienced frequent exacerbation of BA, and short-term oral corticosteroid bursts were occasionally administered. High-resolution CT of the chest revealed diffuse centrilobular nodules with bronchial wall thickening and patchy ground-glass opacities in both lungs. Lung biopsy specimens showed widespread cellular bronchiolitis with follicle formations in the membranous and respiratory bronchioles, accompanied by marked infiltration of plasma cells and eosinophils. In addition, immunohistochemical immunoglobulin G4 (IgG4) staining revealed many IgG4-positive plasma cells, and the ratio of IgG4-positive cells to IgG-positive cells exceeded 40%. The final diagnosis was eosinophilic bronchiolitis with marked IgG4-positive plasma cell infiltration in association with BA. With benralizumab therapy, her clinical condition dramatically improved.
- asthma
- bronchitis
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Eosinophilic bronchiolitis (EB) was first reported as chronic bronchiolitis with eosinophilic lung disease by Takayanagi et al.1 It is often associated with bronchial asthma (BA) or eosinophilic pneumonia. BA is the disorder that most commonly accompanies EB.
Increased levels of immunoglobulin G4 (IgG4) are known to be associated with allergic reactions. However, little is known about implications and role of increased IgG4 levels.2 Flament et al reported that several patients with BA had elevated serum IgG4 levels, and those patients had higher blood levels of eosinophils and total IgE levels and higher fractions of exhaled nitric oxide (FeNO).3 According to some studies, patients with IgG4-related diseases and allergic diseases share a common immune system response, including predominantly a Th2-type cytokine response. It is assumed that levels of a Th2-type cytokine interleukin-10 are related to the production of IgE and IgG4.4–6 Thus, IgG4-positive plasma cells may play a role in the pathogenesis of bronchiolar diseases associated with BA.
We report a case of long-term efficacy and safety of benralizumab in a patient with BA who had EB in association with marked IgG4-positive plasma cell infiltration.
Case presentation
A 53-year-old non-smoking Japanese woman was admitted to our hospital with a 20-year history of wet cough and dyspnoea on exertion. BA had been diagnosed 20 years earlier. Although she has been treated with high-dose inhaled corticosteroid, a long acting β2 agonist and a leukotriene receptor antagonist, she experienced frequent exacerbations of BA, and short-term oral corticosteroid bursts were occasionally administered. Her FeNO was elevated (53 ppb). Blood tests revealed eosinophilia (3480 /µL) and a high total IgE level (353 IU/mL). High-resolution CT (HRCT) of the chest revealed diffuse centrilobular nodules and bronchial wall thickening in both lungs. In addition, patchy ground-glass opacities were observed around the bronchioles (figure 1A,B). The pulmonary function test demonstrated obstructive impairment (forced expiratory volume in 1 s (FEV1): 1.55 L, 65.7%; coefficient G for the ratio of FEV1 to forced vital capacity: 57.8%; the ratio of residual volume to total lung capacity (RV/TLC): 43.3% with airflow obstruction). The result of bronchodilator reversibility testing was positive.

Serial changes in high-resolution CT (HRCT) of the chest. (A and B) At the initial visit, HRCT revealed diffuse centrilobular nodules and bronchial wall thickening in both lung fields. In addition, patchy ground-glass opacities were observed around the bronchioles. (C and D) Three months after benralizumab and high-dose inhaled corticosteroid therapy began; the diffuse centrilobular nodules and ground-glass opacities in both lung fields were markedly improved. (E and F) Six months after the start of therapy, HRCT of the chest showed further improvement, but an area of thin-walled bronchiectasis remained unchanged.
Differential diagnosis
Possible causes of diffuse centrilobular nodules suggestive of bronchiolitis include inflammatory conditions, neoplastic disorders, allergic disorders such as EB and eosinophilic granulomatosis with polyangiitis (EGPA), and allergic bronchopulmonary aspergillosis (ABPA), drug causes, autoimmune disorders such as Sjögren’s syndrome, rheumatoid arthritis, and IgG4-related diseases and miscellaneous disorders such as diffuse panbronchiolitis and sarcoidosis. Examination of bronchoalveolar lavage fluid revealed an elevated percentage of eosinophils (49.4%). Our patient had no history of new drug use or other autoimmune disorders. All tests of autoimmune antibodies and tumour markers yielded negative results. Cultures of sputum and bronchoalveolar lavage fluid were negative for fungal, bacterial and mycobacterial pathogens. The diagnosis of EGPA proposed by the American College of Rheumatology requires four of the following six criteria: asthma, a high eosinophil level (>10%), neuropathy, pulmonary infiltrates, paranasal sinus disease and extravascular eosinophils.7 Our patient had no history of neuropathy, chronic paranasal sinusitis or extravascular eosinophils. Moreover, there was no evidence of specific IgE to Aspergillus antigen and characteristic radiological findings, including mucoid impaction or central bronchiectasis, as seen in ABPA. Therefore, we decided to perform video-assisted thoracic surgery.
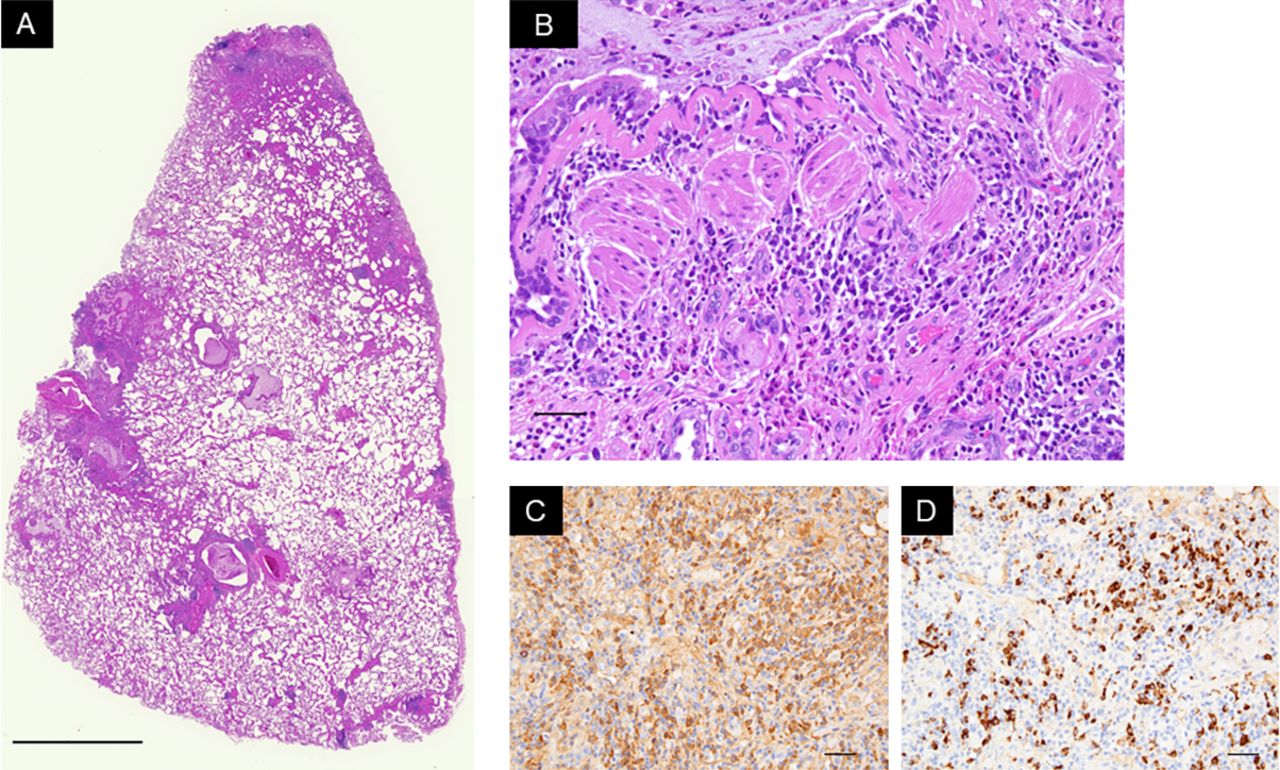
Lung biopsy specimens showed widespread cellular bronchiolitis with scattered follicle formations in membranous and respiratory bronchioles, accompanied by marked infiltration of small round cells, predominantly plasma cells and eosinophils, as well as mucous retention and thickened basement membrane (figure 2A,B). In addition, immunohistochemical staining showed many IgG4-positive plasma cells and an increased ratio of IgG4-positive cells to IgG-positive cells (>40%; Figure 2C,D). We found no convincing evidence of accumulation of foamy macrophages in respiratory bronchioles, scattered non-caseating epithelioid cell granulomas, obliterative phlebitis or arteritis, storiform fibrosis, or neoplastic cells. Additional serological studies demonstrated elevated levels of IgG4 (214 mg/dL). The histopathological diagnosis was EB with marked IgG4-positive plasma cell infiltration in association with BA.
{kind=link}
{kind=link}
Histopathological findings of lung biopsy specimens obtained by video-assisted thoracoscopic surgery. (A) Low magnification microscopic appearance of the right upper lobe revealed widespread cellular bronchiolitis with follicle formations in the membranous and respiratory bronchioles (H&E stain; bar represents 1 cm). (B) High magnification microscopic appearance of the right lower lobe. Note intraluminal mucus retention and thickened basement membrane, as well as infiltration of marked small round cells, predominantly plasma cells and eosinophils (H&E stain; bar represents 50 µm). (C) Immunohistochemical staining of immunoglobulin G (IgG; bar represents 50 µm). (D) Immunohistochemical staining of immunoglobulin G4 (IgG4; bar represents 50 µm) revealed many IgG4-positive plasma cells; the ratio of IgG4-positive cells to IgG-positive cells exceeded 40%.
Treatment
The patient did not accept systemic corticosteroid therapy. We initiated treatment with benralizumab because she had uncontrolled BA and airflow obstruction despite treatment with high-dose inhaled corticosteroids.
Outcome and follow-up
Three months after combination treatment with benralizumab and high-dose inhaled corticosteroid began, the patient’s respiratory symptoms and chest HRCT abnormalities, such as diffuse centrilobular nodules and ground-glass opacities in both lung fields, markedly improved (figure 1C,D). Six months after therapy began, HRCT of the chest showed further improvement, but an area of thin-walled bronchiectasis remained unchanged (figure 1E,F). The value of FEV1 decreased from 1.55 L to 2.50 L, and the ratio of RV/TLC decreased from 43.3% to 26.9%. In addition, the FeNO decreased from 53 ppb to 29 ppb. No exacerbation or adverse effects were observed in the subsequent 12 months.
Discussion
To the best of our knowledge, this is the first reported case of EB with marked IgG4-positive plasma cell infiltration in association with BA that was successfully treated with benralizumab.
EB was first reported as chronic bronchiolitis with eosinophilic lung disease by Takayanagi et al.1 In 2013, Cordier et al described this condition as hypereosinophilic obliterative bronchiolitis, defined by (1) blood hypereosinophilia >1000/μL or eosinophilia in bronchoalveolar lavage fluid (>25%), or both, (2) airflow obstruction despite treatment with high-dose inhaled bronchodilators and corticosteroids and (3) characteristic signs of bronchiolitis on HRCT of the chest or EB in lung biopsy specimens.8 Our patient’s manifestations fulfilled these criteria for EB. EB is often associated with BA or eosinophilic pneumonia, and BA is the disorder that most commonly accompanies EB.
Increased levels of IgG4 are known to be associated with allergic reactions. However, the implications of increased IgG4 level and its role in disease are not well known.2 Zen and Nakanuma reported that in 12% of patients with IgG4-related diseases, BA had been diagnosed.9 Flament et al reported that several patients with BA had elevated serum IgG4 levels, and those patients also had higher blood levels of eosinophils and total IgE and FeNO values.3 The authors speculated that the level of the Th2-type cytokine interleukin-10 is related to the production of IgE and IgG4.4–6 Moreover, Jeannin et al found that Th2-related cytokines could induce the switch from IgE to IgG4.10 Thus, IgG4-positive plasma cells may play a role in the pathogenesis of bronchiolar diseases associated with BA. We think that it is difficult to clinically distinguish an increase in IgG4-positive plasma cells derived by expression of Th2-type cytokines in BA from IgG4-related diseases.
In our patient, we diagnosed EB with marked IgG4-positive plasma cell infiltration in association with BA, and we treated her with benralizumab because she had uncontrolled BA and airflow obstruction despite treatment with high-dose inhaled corticosteroids. Benralizumab is an interleukin-5 receptor monoclonal antibody licensed for the treatment of severe eosinophilic BA. In clinical trials, it has demonstrated efficacy in reducing rates of asthma exacerbation and in reducing the need for maintenance oral corticosteroids.11 12 There is little evidence regarding the appropriate treatment for EB. In general, inhaled high-dose corticosteroids alone are not adequate in patients with EB. Although oral corticosteroid therapy is usually effective, tapering the dosage often leads to relapse. Takeshita et al reported a patient in whom mepolizumab was successful in the treatment of EB.13 Since our patient refused systemic corticosteroid therapy, we decided to start treatment with benralizumab. Her symptoms, chest abnormalities and pulmonary function test findings dramatically improved. Benralizumab may, thus, be a promising strategy for the treatment of EB.
Patient’s perspective
I had suffered from severe bronchial asthma and received occasionally short-term oral corticosteroid bursts due to awful asthma attack for more than 20 years. No sooner had I received benralizumab than I felt improvement immediately. I am greatly happy to meet an appropriate noble therapy.
Learning points
Eosinophilic bronchiolitis (EB) should be on the list of differential diagnoses for patients presenting with poorly controlled bronchial asthma (BA), persistent serum eosinophilia and diffuse centrilobular nodules suggestive of bronchiolitis.
A combination of clinical and histopathological findings is required for the diagnosis of EB.
While not commonly seen in BA with EB, consider a diagnosis of immunoglobulin G4 related disease.
Benralizumab may be a promising strategy for the treatment of EB.
Ethics statements
Patient consent for publication
References
Footnotes
Contributors KS, HO, AH and ET drafted the manuscript. All authors read and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.