Article Text

Statistics from Altmetric.com
Description
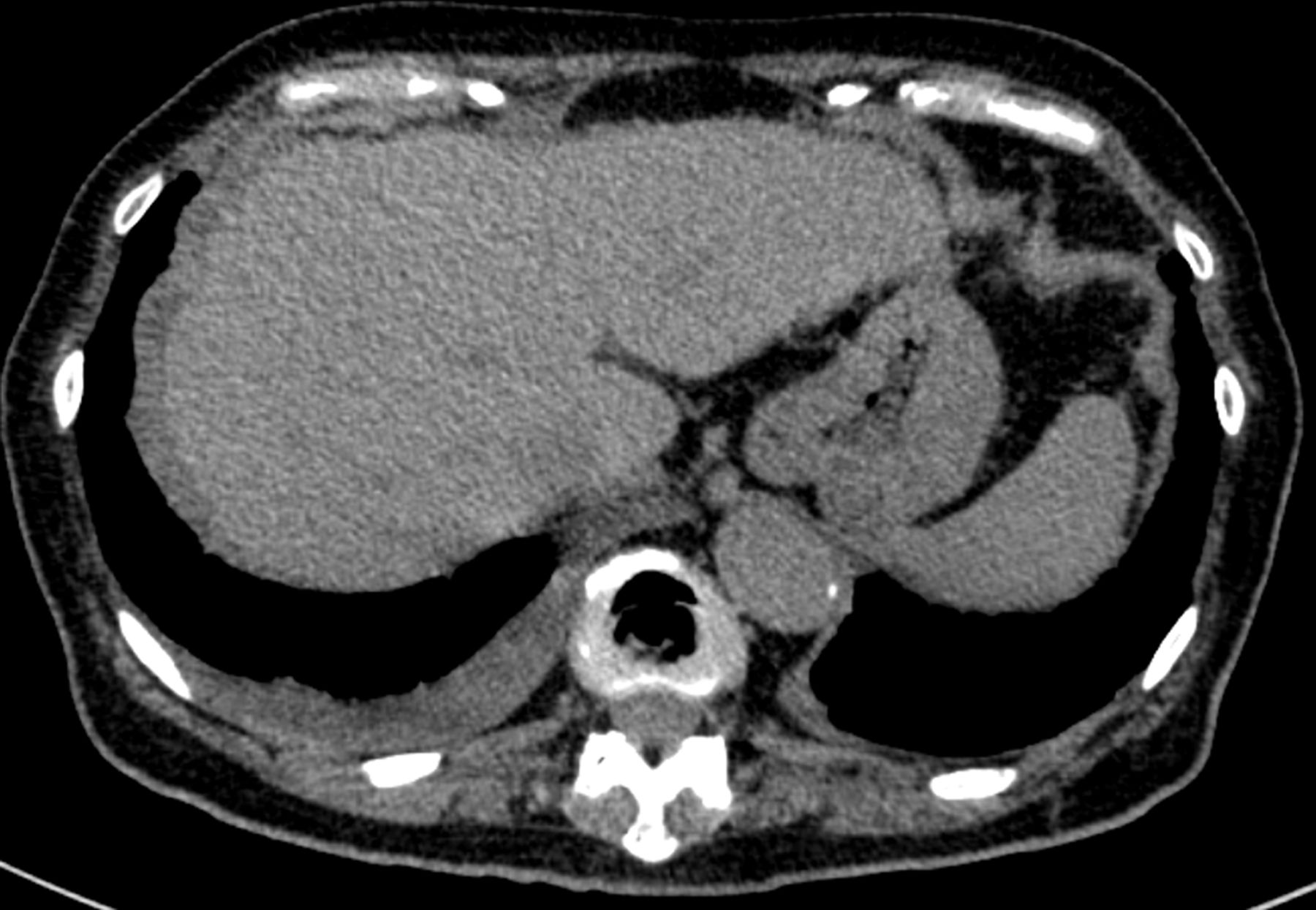
The patient was a 77-year-old woman who had undergone surgery for gastric cancer, and who had periodically received CT of the chest and abdomen. At 7 years after the operation, CT revealed ascites with uniform peritoneal thickening and a small amount of unilateral pleural effusion (figure 1). Based on these CT findings, the attending surgeon suspected a recurrence of gastric cancer with systemic dissemination, including carcinomatous peritonitis. Exploratory laparoscopy revealed tiny yellow/white nodules diffusely covering the surface of anterior peritonea (figure 2) and small bowel. Histology was negative for malignancy but Ziehl-Neelsen staining was positive for acid-fast bacilli in non-caseating granulomas. Furthermore, the pleural fluid showed lymphocytosis with elevated levels of adenosin deaminase. An interferon-gamma release assay was positive. Based on these findings, although the patient did not have a distinct history of tuberculosis, we diagnosed her with miliary tuberculosis, including tuberculous peritonitis.

CT showing ascites with uniform peritoneal thickening and a small amount of right pleural effusion.

{kind=link}
{kind=link}
A laparoscopic photograph, showing tiny yellow/white nodules diffusely covering the surface of the anterior peritoneum.
Tuberculous peritonitis is a rare form of tuberculosis that involves the parietal and visceral peritoneum, omentum and intestinal mesentery.1 The possibility of miliary tuberculosis should be considered when ascites with peritoneal thickening is present along with pleural effusion.2 A delay in the diagnosis and treatment of tuberculosis increases patient mortality, suggesting that an early diagnosis by laparoscopic biopsy is very important for a prompt diagnosis and initiation of treatment.3
Patient’s perspective
I will be glad to be of help for the future healthcare.
Learning points
When ascites with peritoneal thickening is present along with pleural effusion in a patient with cancer, not only progression of the cancer but also miliary tuberculosis should be considered.
An early diagnosis by laparoscopic biopsy is important for a prompt diagnosis and initiation of treatment for tuberculous peritonitis.
Ethics statements
Patient consent for publication
Footnotes
Contributors HK and HI researched the topic and wrote the case. RS and YK helped with the research and proofreading of the case report.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.