Article Text

Statistics from Altmetric.com
Description
A 2-year-old child presented to the paediatric emergency department with sudden onset of inability to stand unsupported for 1 week. The parents noticed a discharging sinus in posterior aspect of lower neck at 2 months of age, which had discharged pus 2 months ago, with associated fever and pain. At presentation, there was no discharge or fever. On examination, the child was afebrile with stable vitals. Local examination revealed a midline sinus opening over the upper dorsal spine. No discharge or erythema was seen.
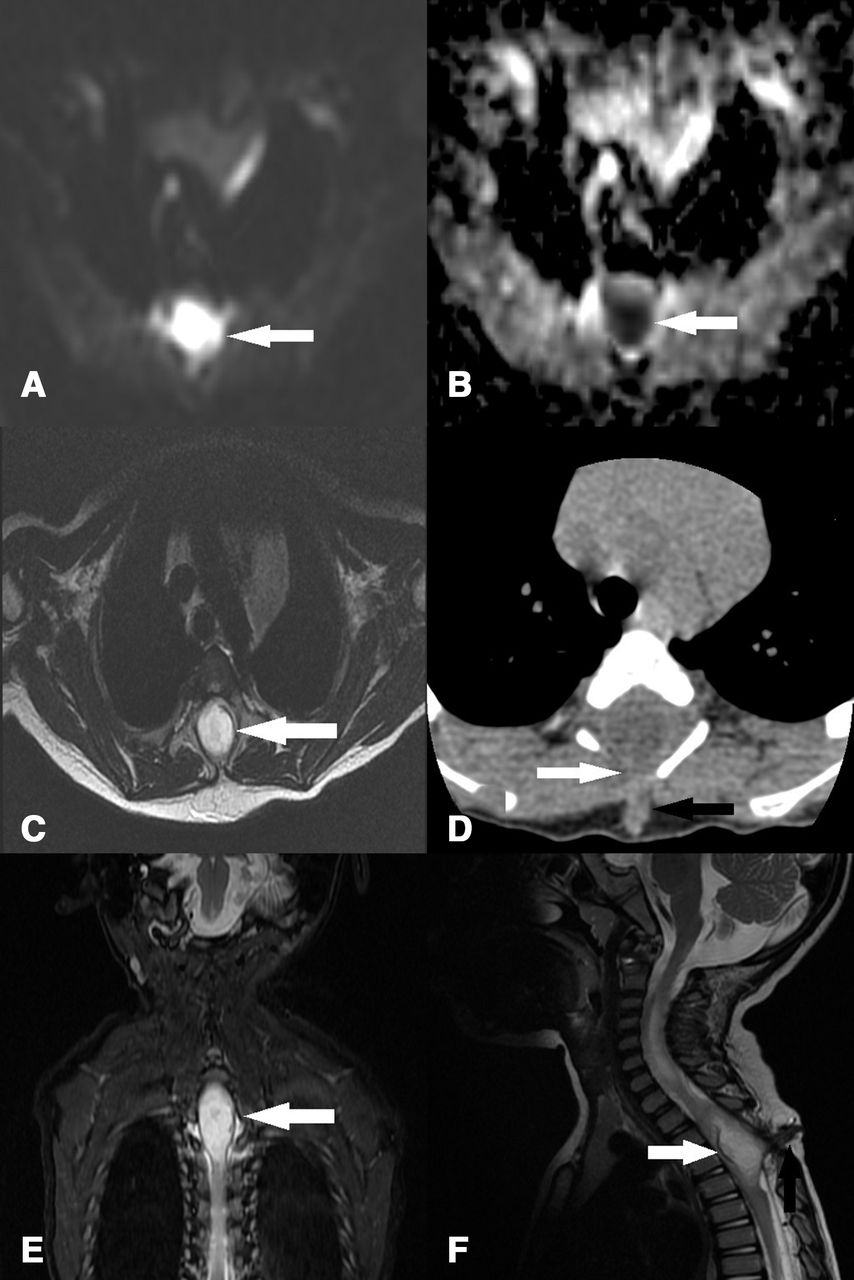
Contrast-enhanced MRI of the spine was performed. Precontrast images demonstrate intramedullary T2 hyperintense lesion with diffusion restriction and perilesional oedema at D3–D6 (figure 1A-F). A dorsal dermal sinus tract communicating with the spinal canal was noted at D4 level (figure 2A,B). Lesion showed rim enhancement (figure 2C,D) on postcontrast images. Tethered cord (figure 2E,F) was also noted. CT of dorsal spine revealed absent posterior vertebral process of D3–D5 vertebrae (figure 1D). Radiological diagnosis of intramedullary abscess was made. The child underwent myelotomy with drainage of abscess, excision of the lesion and dermal sinus with untethering of cord. Intraoperatively, diagnosis of infected dermoid sinus was made, and the same was confirmed by histopathological examination.
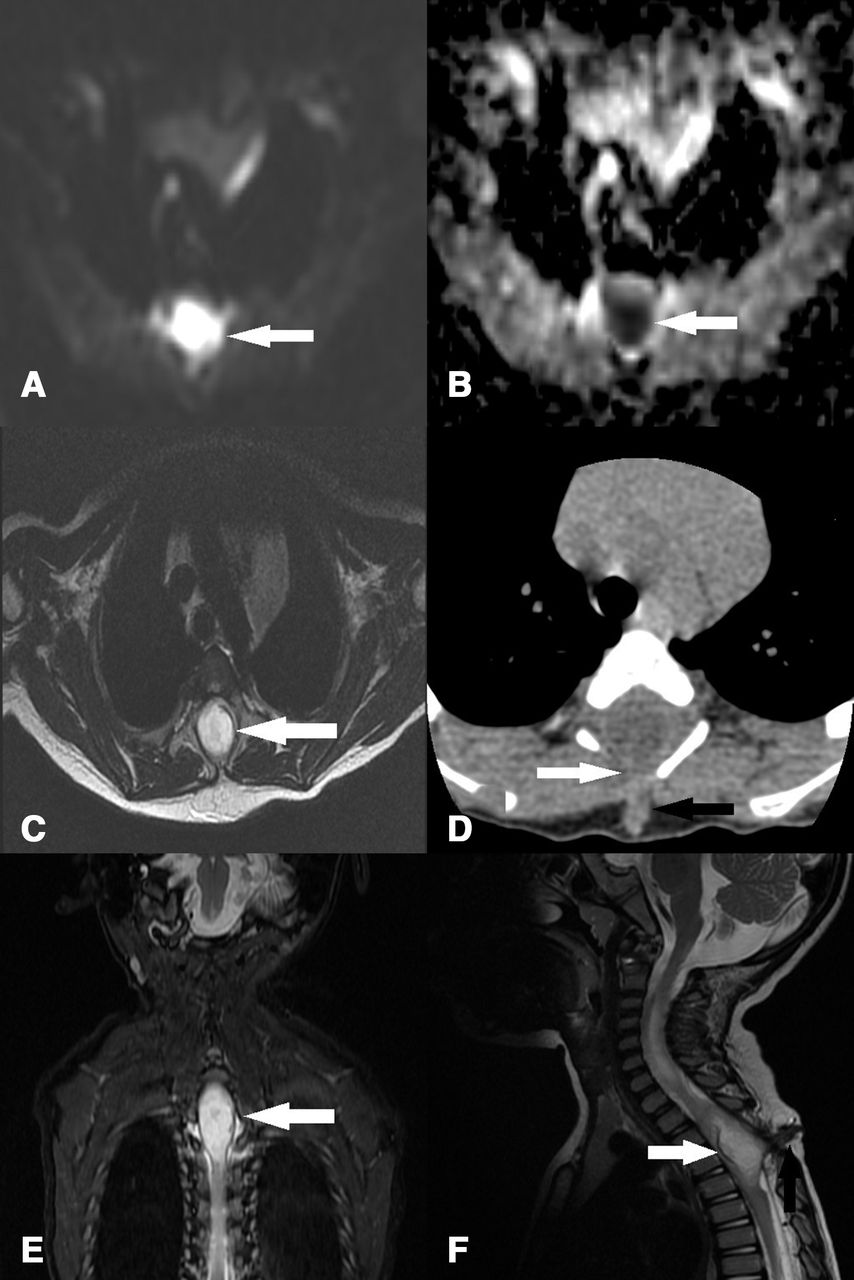
A, B: Diffusion Weighted Image (DWI) and Apparent Diffusion Coefficient (ADC) images at the level of lesion demonstrating diffusion restriction (white arrow). C: T2-weighted image demonstrating T2 hyperintense intramedullary lesion. D: CT image at the level of D4 vertebra demonstrating absent posterior process of the vertebra (white arrow) and sinus tract (black arrow). E, F: Coronal and sagittal T2-weighted images demonstrating intramedullary hyperintense lesion at the level of D3–D5 vertebrae (white arrow).

{kind=link}
{kind=link}
A, B: Axial and coronal Fast Imaging Employing Steady-sTate Acquisition (FIESTA) images demonstrating hyperintense intramedullary lesion (white arrow) and sinus tract (black arrow). C, D: Sagittal T1 precontrast and postcontrast images demonstrating peripherally enhancing T1 hypointense intramedullary lesion. E, F: Sagittal T2-weighted images demonstrating thickened filum terminale (white arrows)—S/o tethered cord.
Dermal sinus is caused by failure of cleavage of cutaneous ectoderm from neuroectoderm; they can be potential route for infection.1 Dermal sinus accounts for 48% of intramedullary abscess in paediatric population.2 3 The inner end of the dermal sinus can expand and give rise to dermoid or epidermoid tumour1; epidermoid tumours occur more often than dermoid, but dermal sinus is more frequently associated with dermoid.4 5
Intraspinal dermoid cyst accounts for 0.8%–1.1% of intraspinal tumours. They commonly occur in the lumbosacral region and may or may not be associated with spinal dysraphism.6 Dermoid cyst contains dermal and epidermal derivatives; they arise from totipotent ectodermal cells.7 Infected dermoid cyst is a rare cause of intramedullary abscess and can be caused by contiguous spread of infection via dermal sinus.2 3 On MRI, dermoid cyst has heterogenous appearance depending on the content of the cyst.8 Fat content within the cyst can appear hyperintense on T1-weighted image and as a low attenuation lesion on CT.9 The dermal sinus will appear as T1 hypointense tract from the skin to intramedullary region through a defect in posterior element. Infected dermoid cyst has a heterogenous appearance; however, they usually present as a mass causing expansion of cord with perilesional oedema. On postcontrast MRI, there is rim enhancement with features of solid component and septations.10
Treatment of choice is excision of dermal sinus with drainage of abscess through a dorsal midline myelotomy at the site of maximum swelling and fluctuation followed by excision of lesion.1 11 Non-infected dermoid has excellent prognosis, and in case of infected dermoid cyst, only 20% of case could recover completely.2 12 13 Hence, early diagnosis and prompt surgical management of intramedullary abscess are required to prevent complications.
Learning points
Dermoid sinus more often presents with dorsal dermal sinus.
Dorsal dermal sinus can act as pathways for infection leading to formation of intramedullary abscess.
Common location for dermoid cyst is the lumbosacral region.
Ethics statements
Patient consent for publication
References
Footnotes
Contributors DA, KS and JJ have equally contributed to procurement of images, interpretation and clinical follow-up. DA drafted the manuscript; KS and JJ have edited and finalised the draft.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.