Article Text

Statistics from Altmetric.com
Description
A 23-year-old previously healthy north African young man, presented with multiple small calcified yellowish painless lesions of 5 mm to 1.5 cm covering most of his scrotum that have been progressively appearing for over 15 years with simultaneous depigmentation of the scrotum (figure 1). Physical examination found amelanotic lesions affecting the scrotum, the glans of the penis, with two small patches on the areolas and nipples. There was no pain or discharge and the patient never seeked medical assistance as it was practically asymptomatic.

Multiple painless nodules involving scrotum with large well-limited depigmentation consistent with stable vitiligo.
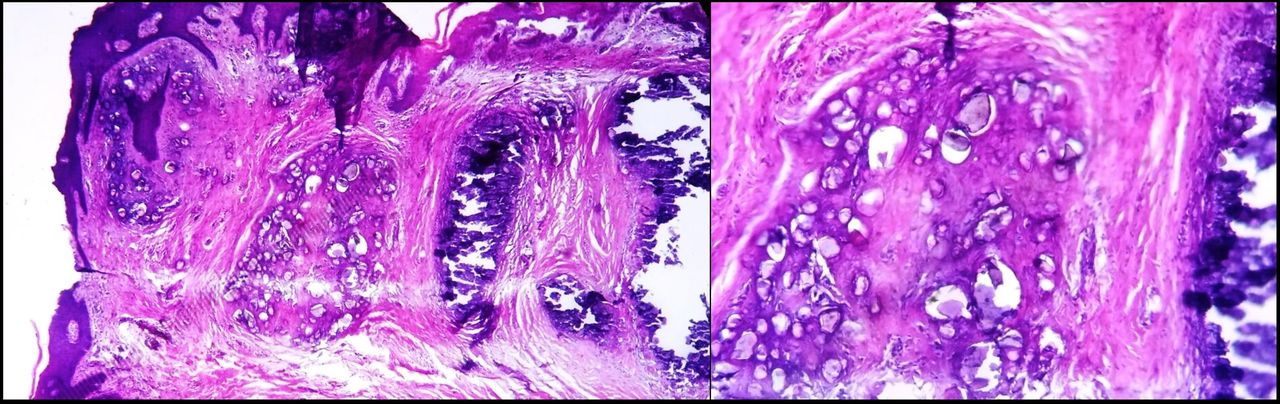
Laboratory tests including serum calcium and phosphorus were normal. Histological examination of a skin biopsy confirmed the diagnosis of scrotal calcinosis (figure 2). After informed consent, a total excision of the affected scrotal skin and primary closure was performed, resulting in a good aesthetic outcome.
{kind=link}
{kind=link}
Histological examination revealing aggregates of calcium in the dermis consistent with scrotal calcinosis.
Scrotal calcinosis is a very rare and benign condition; occurring in the absence of metabolic and phosphocalcic disorders. It was described for the first time by Lewinski in 1883.1 The association with vitiligo was previously described once by Feinstein et al in 1984.2
Scrotal calcinosis usually affects young African men aged 20 to 40 years old. It clinically manifests as firm yellowish usually multiple nodules that may spread on the whole penoscrotal area. Their size varies from few millimetres to several centimetres. The condition is generally asymptomatic; in some rare cases it can cause itching or pelvic and perineal pain. Histological examination in scrotal calcinosis usually finds calcium deposits in the dermis with no epithelial lining.2 3
Surgical treatment remains the mainstream in the management of scrotal calcinosis. The main purpose of surgery is to improve the aesthetic appearance of the scrotum. The surgical excision must be limited to the scrotal skin since the calcifications are limited to the dermis. Generally, even in case of extensive lesions, primary closure of the defect is possible due to the important elasticity of the scrotal skin. In case of impossible primary closure, multiple options are possible such as skin grafting or musculocutaneous flaps. The relapse incidence is unknown. Some authors suggest that complete surgical excision of all the calcified nodules including the smaller ones prevents recurrences.3
The pathogenesis of scrotal calcinosis is mostly speculative. Some believed that the lesions are caused by dystrophic calcification of the dartos muscles of the scrotum.4 The role of repeated minor trauma has also been suggested.2 In our case, association with vitiligo, which is known to be triggered by Keobner phenomenon, on the same area may reinforce this hypothesis.
However, most recent and well documented data suggest that the calcified lesions are probably the result of dystrophic calcification in the wall of epithelial cysts. In fact, in many patients with supposedly « idiopathic » scrotal calcinosis, especially young patients below 30 years of age, epithelial cysts with a variable amount of keratin and calcification or epithelial remnants were found along with the fully developed lesions of scrotal calcinosis, suggesting that the calcification of these epithelial cysts is probably the main cause of scrotal calcinosis.5
Learning points
Scrotal calcinosis is a rare benign condition that can be, aesthetically and psychologically, very disturbing.
In our case, the association with vitiligo made it even harder on our young patient to have a normal sexual life.
The exact cause of this association (microtrauma, Keobner phenomenon…) remains a mystery.
Footnotes
Contributors SM: contributed in conception, design and drafting of the article, participated in patient’s care. HD: contributed in conception, design and drafting of the article, participated in patient’s care. LB: contributed in patient’s care. KS: supervised all the decisions concerning the patient and the writing process.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.