Article Text

Statistics from Altmetric.com
Description
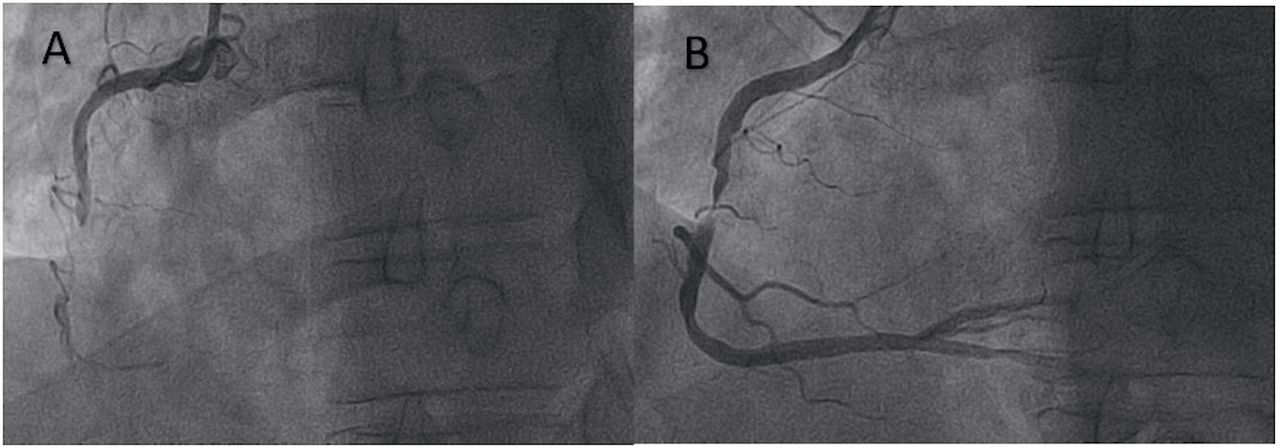
A 46-year-old man presented to the hospital with a brutal chest oppression with mandibular and left arm discomfort. He was a current smoker (28 pack-year) and his father had experienced a myocardial infarction. He was not receiving any medical treatment. The first ECG showed an inferior ST-elevation myocardial infarction (STEMI). Angiography revealed a mid-right coronary artery occluded by a thrombus (figure 1A), treated by angioplasty. He had an uneventful evolution after angioplasty in the coronary care unit and a normal left ventricular ejection fraction. His body mass index (BMI) was 26.6 kg/m2, his low-density lipoprotein cholesterol (LDL-C) level was 121 mg/dL and triglyceride level was 233 mg/dL. No other risk factors were identified.
{kind=link}
Coronary angiogram of inferior myocardial infarction showing mid-right coronary artery occlusion for the first twin (A) and a subocclusion at the same site for the second twin (B).
One year and 4 months later, his monozygotic twin brother was admitted to the hospital due to a sudden onset of chest pain and dyspnea. He was a former smoker (25 pack-year) taking aspirin and atorvastatin 10 mg since his brother’s infarction. The prehospital ECG showed an inferior STEMI. Coronary angiography disclosed mid-right coronary subocclusion and images suggestive of intracoronary thrombus (figure 1B). Angioplasty was performed with a drug-eluting stent implantation in the mid-right coronary artery, followed by resolution of electrocardiographic signs and symptoms. His BMI was 25.2 kg/m2, LDL-C level was 51 mg/dL and triglyceride level was 260 mg/dL under atorvastatin. Lipoprotein (a) level was 124 mg/dL. No other risk factors were identified.
Both twin patients exhibited a very similar coronary artery disease, at the same age, with a very close coronary anatomy and an acute unstable coronary lesion in the mid-right coronary artery. This highlights a high concordance in coronary anatomy between monozygotic twins, between evident genetic factors and close environmental data.1 2
Learning points
There is a high concordance in coronary anatomy between monozygotic twins, between evident genetic factors and close environmental data.
It reinforces the importance of primary prevention and thorough screening in twins’ siblings, when one is suspected of coronary disease.
Footnotes
Contributors AC drafted the manuscript and took care of the patient. FP drafted and revised the manuscript and took care of the patient. OV drafted and revised the manuscript and took care of the patient.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.