Article Text

Statistics from Altmetric.com
Description
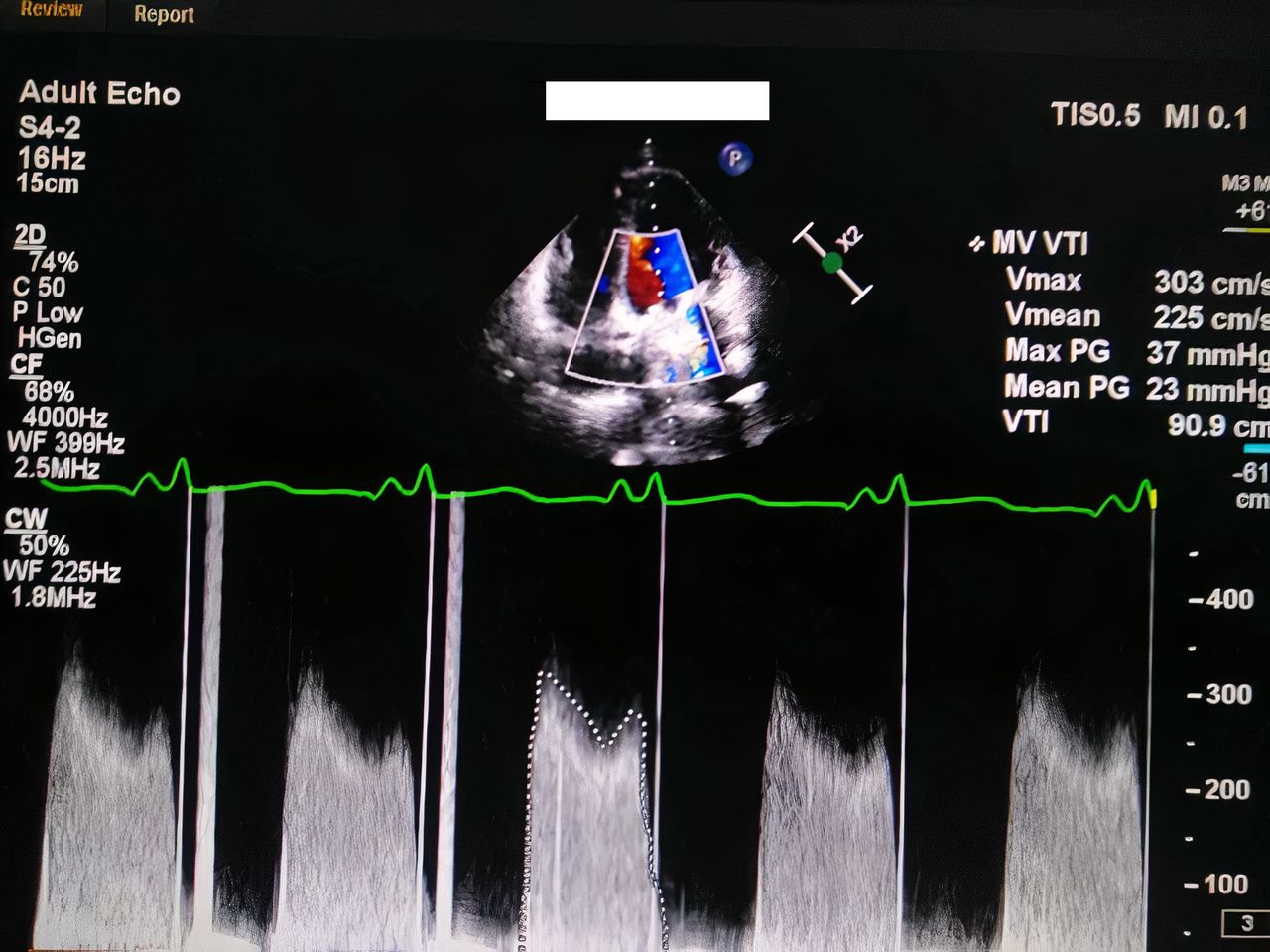
A 39-year-old, G3 F1 P0 A1 L1 with one prior vaginal delivery, was referred to our obstetrics outpatient clinic (OPC) with the diagnosis of missed abortion at ±8 weeks of gestational age (GA) for surgical evacuation. Her history was significant for rheumatic heart disease on long acting penicillin as well as that she underwent open heart surgery with mitral mechanical valve replacement (MVR) (sorin bicarbon bileaflet 25’) 4 years prior. She had been on vitamin K antagonist (VKA) 5 mg daily since MVR with good international normalised ratio (INR) control; then, her obstetrician and referring physician shifted her to unfractionated heparin (UFH) 5000 IU two times daily since the diagnosis of pregnancy. Surprisingly, she instructed her to discontinue the UFH during her last follow-up visit 2 days before, when missed abortion was diagnosed by ultrasound. The patient was slightly dyspnoeic and reported palpitations. Accordingly, she was admitted at our high risk pregnancy unit and subsequently had an urgent consultation with the cardiology team, who performed a transthoracic echocardiogram (TTE) that showed mechanical valve peak and mean transvalvular pressure gradients (PGs) at 37 and 23 mm Hg, respectively (figure 1), while the normal peak and mean PGs for the valve type and size are 15±3 and 5±1 mm Hg, respectively. As emergency transoesophageal echocardiogram (TOE) was not available then, the cardiology team opted for fluoroscopy that showed complete immobility of one of the valve leaflets (video 1). The patient was urgently transferred to the cardiothoracic surgery service where she had a redo mitral MVR (St. Jude medical bileaflet 25’) surgery after preparation. Postoperatively, she had a smooth recovery in the coronary intensive care unit (CCU). A week later, medical evacuation was induced using vaginal misoprostol 600 mg*three under strict monitoring in the CCU. She delivered the dead fetus, while the retained products of conception (RPOC) necessitated transference to our service for dilatation and suction evacuation of RPOC in the operation room. She was on UFH for anticoagulation that was stopped 6 hours before operation and then resumed postoperatively in the CCU. She was restarted on VKA under UFH cover until they obtained an INR control between 2.5 and 3.5 and then they stopped UFH and continued on VKA. Again, her recovery was smooth, she was transferred to the floor and then discharged home. She has been following up regularly with the cardiology OPC since then, who referred her lately to the gynaecology OPC to insert a hormonal intrauterine device (IUD) for contraception.
{kind=link}
TTE with colour Doppler showing high mean and peak transvalvular pressure gradients. TTE, transthoracic echocardiogram.
Pregnancy with MVR is a very high risk one, with uneventful pregnancy occurring only in 28%–58% of patients. Valve thrombosis occurred in 4.7% of patients in one study and was associated with 20% mortality rate, while the overall mortality rate due to valvular complications was 9% of all MVR patients in another one.
VKA is the most effective therapy to prevent prosthetic valve thrombosis during pregnancy, though it is associated with high risk of fetal anomalies and fetal loss, particularly if doses exceeded 5 mg/day. Thus, some clinicians prefer shifting to low molecular weight heparin (LMWH) or UFH, especially in the first trimester (as in our case). This shift occurs again at 36 weeks of GA, as VKA has long half-life that can cause significant haemorrhage if preterm delivery occurs.1
In discordance with the European Society of Cardiology guideline,1 we follow the American Heart Association (AHA) and American College of Cardiology (ACC) guideline recommendations in this point, that anticoagulant with VKA should be administered with aspirin 75–100 mg once a day.2 Optimally, therapeutic doses of VKA should be monitored weekly with INR target of 3, UFH with activated partial thromboplastin time ≥2 times the control value, and LMWH with anti-Xa level 1–1.2 unit/mL.1
Even though surgical evacuation is safer, faster and slightly more effective than medical evacuation, missed abortion is not a surgical emergency.3 Stopping UFH after abortion without planning for surgery within the next 6 hours to evacuate the conceptus was an absolute iatrogenic error.2 Hormonal IUD is the best and safest contraception for MVR patients.1
Prosthetic valve obstruction is defined as mean transvalvular PG increase of >50% relative to the baseline, or above established normal values for the type and size of valve if a baseline echo is not available (as in our case). Severe obstruction is suggested by mean gradient >10 mm Hg.4
Even though TTE allowed assessment of valve and cardiac chambers functions, and fluoroscopy clearly visualised absent motion of one of the valve leaflets, performing TOE as a part of multimodality imaging could have been appropriate for confirming the obstruction with good assessment of the thrombus size, location and extent, as well as the aforementioned functions.2 5
Although redo surgery was the optimal management for our patient, AHA/ ACC recent guideline update showed high efficacy and safety with the ‘echocardiogram-guided slow-infusion low-dose fibrinolytic therapy’ protocol. Redo surgery was a better choice for our patient based on the absence of contraindications to surgery, with the availability of the facilities and surgical expertise, while we had no experience with the later protocol.2 Conservative management with optimal anticoagulation therapy and follow-up is rarely indicated and is rarely successful, it may be attempted only in patients who are not critically ill, with small recent thrombus visualised on TOE, and history of recent inadequate anticoagulation. Failed conservative management is a call for definitive management with redo surgery or thrombolytic therapy.1
Mechanical MVR was a better choice for our patient than bioprosthetic valve. That is based on patient’s young age, absence of contraindications to VKA, good compliance and patient’s desire to avoid the risk of reintervention.2
Learning points
For safety, in mechanical valve replacement (MVR) patients, anticoagulant doses of low molecular weight heparin needs to be monitored with anti-Xa, unfractionated heparin with activated partial thromboplastin time and vitamin K antagonist with international normalised ratio.
Anticoagulation should never be interrupted in a patient with a MVR, except perioperative, with the use of bridging therapy.
Obstructive valve thrombosis should be suspected in any MVR patient who presents with the mildest symptoms with the history of missing anticoagulation, and urgent evaluation with multimodality imaging is required, followed by therapy accordingly.
Footnotes
Contributors The case was under the care of AM. ITE wrote and edited the manuscript. HG revised it linguistically.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.