Article Text

Statistics from Altmetric.com
Description
This was a 3-year-old boy, of weight 15 kg, with no significant medical history receiving tonsillectomy due to obstructive sleep apnoea. General anaesthesia was induced with midazolam, propofol, remifentanil and cisatracurium, and airway was secured with 4.0 mm oral endotracheal tube. After sevoflurane was introduced to maintain anaesthesia, the peak airway pressure suddenly rose to 45 cmH2O and wheezing breath sounds were auscultated bilaterally. Such symptoms resolved with bronchodilation and antihistamine treatment, and he was extubated after the surgery was cancelled. Overnight he suddenly developed cough and difficulty in breathing, then he coughed out a soft translucent viscous cast shaping as tree branches (figure 1). The chest radiograph showed non-specific atelectasis. The pathological result of the excreted airway cast demonstrated necrotic detachment epithelium and inflammatory exudate, where neutrophils were the main inflammatory cells (figure 2). His allergen-specific IgE test was positive for latex and inhalation anaesthetics, and in vitro basophil activation assay was positive for sevoflurane. The patient was discharged home in post-anaesthesia day 7 with no other complications. There was no evidence of recurrence at follow-up of 3 months.

Bronchial cast removed from the patient, showing the shape of bronchial tree.

{kind=link}
{kind=link}
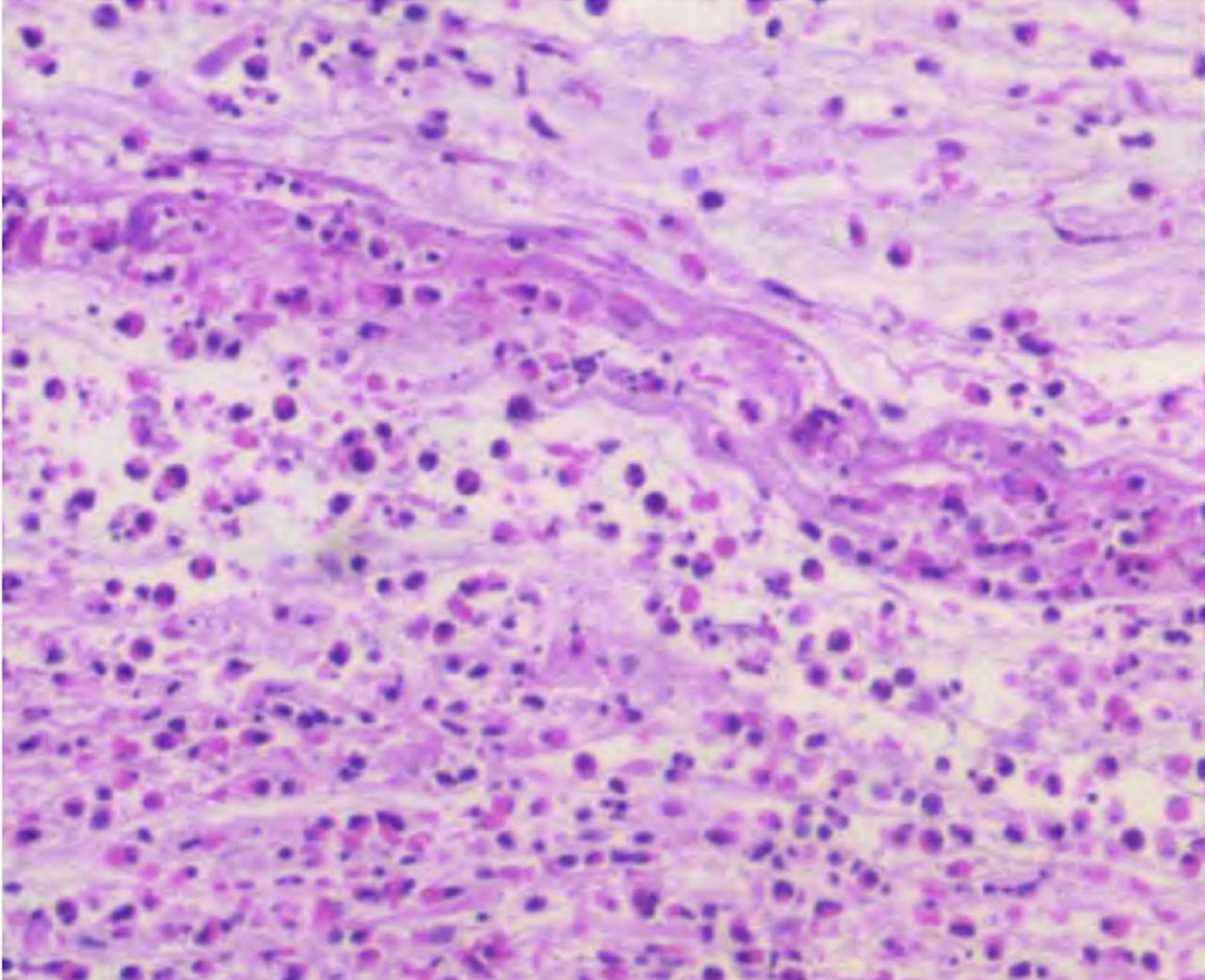
Histology of the excreted airway cast, demonstrating necrotic detachment epithelium and inflammatory exudate.
Plastic bronchitis (PB) is a rare but serious respiratory disease which is characterised by the formation of a plastic foreign matter that leads to partial or extensive obstruction in the respiratory tract. Although PB was first reported over a century ago, its causes still remain unclear.1 The patients present with difficulty in breathing or even respiratory failure.2 The overall incidence of PB is approximately 6.8/100 000, with increased risk among patients with congenital heart disease, pneumonia or influenza and asthma.3 Based on histology PB has been classified into: type I inflammatory cell type, characterised by numerous inflammatory cells (mainly of eosinophils and neutrophils) and cellulose; type II non-inflammatory cell type, characterised by non-cellular substance (mainly of mucin and little cellulose), which is more common after surgery of congenital heart disease with associated abnormal lymphatic drainage.4 Children with reactive airway disease are more prone to the development of type I cast, and the cause is related to inflammatory reaction and consequent neutrophils and eosinophils infiltration.3 This patient developed airway inflammation due to allergic reaction to the volatile agent sevoflurane, subsequently confirmed by immunology testing. The diagnosis of PB is confirmed by presentation of bronchial cast which is obtained by the patient’s spontaneous coughing, manual suction via the tracheal intubation or by bronchoscopy.5 The expectorated cast by presented patient was composed mainly of inflammatory cells, supporting the diagnosis of type I PB. The treatment of PB focuses on prompt cast removal by bronchoscopy and chronic prevention of cast recurrence. Rigid bronchoscopy and flexible bronchoscopic cryoextraction provide improved airway clearance.6 7 In addition, mucolytics (tissue-type plasminogen activator, heparin, urokinase) and fibrinolytics (acetylcysteine, dornase) have been used by either inhalation or directly instilled via bronchoscope to facilitate cast disruption.2 3 Bronchodilator, inhaled and systemic corticosteroids and azithromycin are commonly used medical therapeutic adjuncts.8 Percutaneous lymphatic embolisation has recently been reported to be effective intervention for PB after surgically corrected congenital heart disease with acquired lymphangiectasia.9
Learning points
The incidence of childhood plastic bronchitis (PB) is rare, yet the onset is usually obscure followed by rapid development.
The clinical manifestations and imaging findings of PB are non-specific, therefore its diagnosis is difficult and mainly based on bronchoscopy and histopathological examination.
Inhaled anaesthetics should not be neglected as a potential trigger when perioperative allergic reactions happen among highly sensitive children.
Footnotes
Contributors Both YQ and RZ wrote and edited the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Parental/guardian consent obtained.
Provenance and peer review Not commissioned; externally peer reviewed.