Article Text

Statistics from Altmetric.com
Description
The authors present an endoscopic endonasal transpterygoid approach for reduction of a lateral recess encephalocele with post-operative cerebrospinal fluid leak. A 43-year-old man presented with right-sided clear rhinorrhea for 2 years. He had no other sinus complaints. On examination, he had a body mass index of 28 and right-sided clear rhinorrhea while leaning his head forward.1 2 This fluid was collected and found to be positive for beta-2 transferrin. The patient was assessed for idiopathic intracranial hypertension (IIH), and he had no evidence of IIH. The patient had no signs of papilloedema on assessment by the neuro-ophthalmology team before or after surgery. The patient had no history of meningitis, trauma, obstructive sleep apnoea or any recent weight changes. CT and MRI of the skull base were obtained (figures 1 and 2). A bony defect was found, the size of the defect was 9.5 mm in maximal diameter. The steps of the transpterygoid technique and reconstruction are explained in detail through video 1.3–14

From minute (0:38–0:50)—a coronal CT study in the bone window demonstrated a right lateral sphenoid sinus skull base defect between foramen rotundum indicated by the red arrow and the vidian canal indicated by the yellow arrow.
{kind=link}
{kind=link}
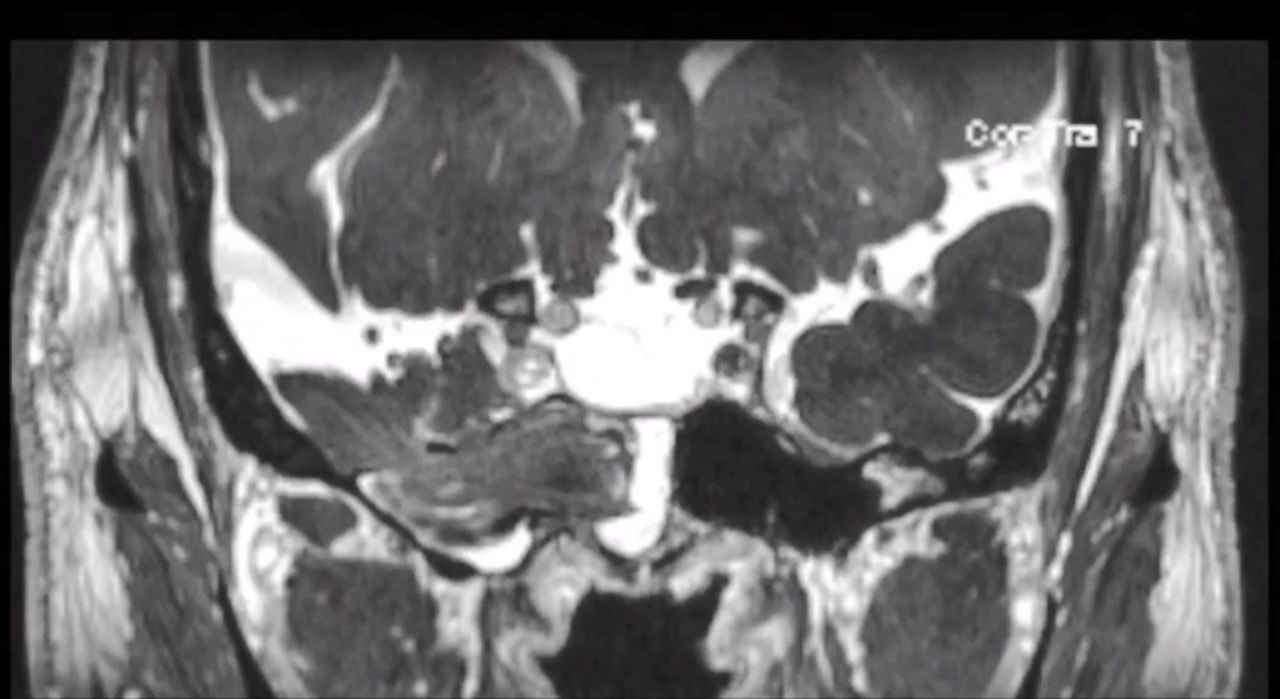
From minute (0:51–0:59)—a T2 weighted coronal MRI demonstrated a large sphenoid sinus encephalocele herniating through a right lateral recess skull base defect.
Postoperatively, the patient refused to adhere to the postoperative bed rest protocol. Sixteen hours after surgery, the patient began to have clear rhinorrhea. The index of suspicion for a cerebrospinal fluid leak was high, and the decision was made to take the patient back to the operating room for re-exploration on postoperative day 2. From this case, we can learn from several technical errors through demonstrating the pitfalls and nuances of the technique. First, full reduction of the encephalocele helps to identify margins of the skull base defect. It is also essential to ensure appropriate preparation of the nasoseptal flap recipient site by skeletonising the skull base, including removal of residual bony edges and removal of sphenoid sinus mucosa. Lastly, we recommend immediate postoperative bed rest and ongoing acetazolamide for our patients following surgical repair of spontaneous cerebrospinal fluid leaks of the anterior skull base.
Learning points
Full reduction of the encephalocele helps to identify margins of the skull base defect.
Ensure appropriate preparation of the nasoseptal flap recipient site by skeletonising the skull base, including removal of residual bony edges and removal of sphenoid sinus mucosa.
Immediate postoperative bedrest and ongoing acetazolamide for patients following surgical repair of spontaneous cerebrospinal fluid leaks of the anterior skull base.
Footnotes
Twitter @KhalafallahAM, @NeuroOncSurgery
Contributors AMK: Conception and design of the case, video creation and editing, writing—original draft, writing—review and editing, final approval of the version published. OGA: Conception and design of the case, video editing, writing—review and editing, final approval of the version published. NRR: Conception and design of the case, writing—review and editing, final approval of the version published. DM: Conception and design of the case, video editing, writing—review and editing, final approval of the version published.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.