Article Text

Statistics from Altmetric.com
Description
A 68-year-old man, a known case of multibacillary leprosy with peripheral neuropathy and arthritis on multidrug therapy (rifampicin 600 mg and clofazimine 300 mg once a month with daily doses of clofazimine 50 mg and dapsone 100 mg) since 3 years with poor compliance and follow-up, defaulted on his therapy since 8 months. He presented with progressive weakness, tingling and numbness of all four limbs in the past 6 months. On examination, he had saddle nose deformity and bilateral claw hand with trophic ulcers. His muscle power was 4/5 proximally and 2/5 distally, with a wasting of small muscles of hands. Triceps and knee reflexes were exaggerated but biceps, brachioradialis and ankle reflexes were diminished bilaterally. Bilateral plantar responses were extensor and he had glove and stocking sensory loss with pseudoathetosis of hands. He also had kinesthetic (vibration and position) sensory loss extending proximally beyond the elbow. MRI of the cervical spine revealed contrast-enhancing swollen cervical dorsal root ganglia suggestive of ganglionitis with T2-weighted hyperintense spinal cord lesion at the C6 level suggestive of myelitis (figures 1 and 2). The patient was reinitiated on multidrug therapy with prednisolone (1 mg/kg), gradually tapered over 6–8 weeks. He reports significant improvement in sensory symptoms and handgrip at 8 months of follow-up.
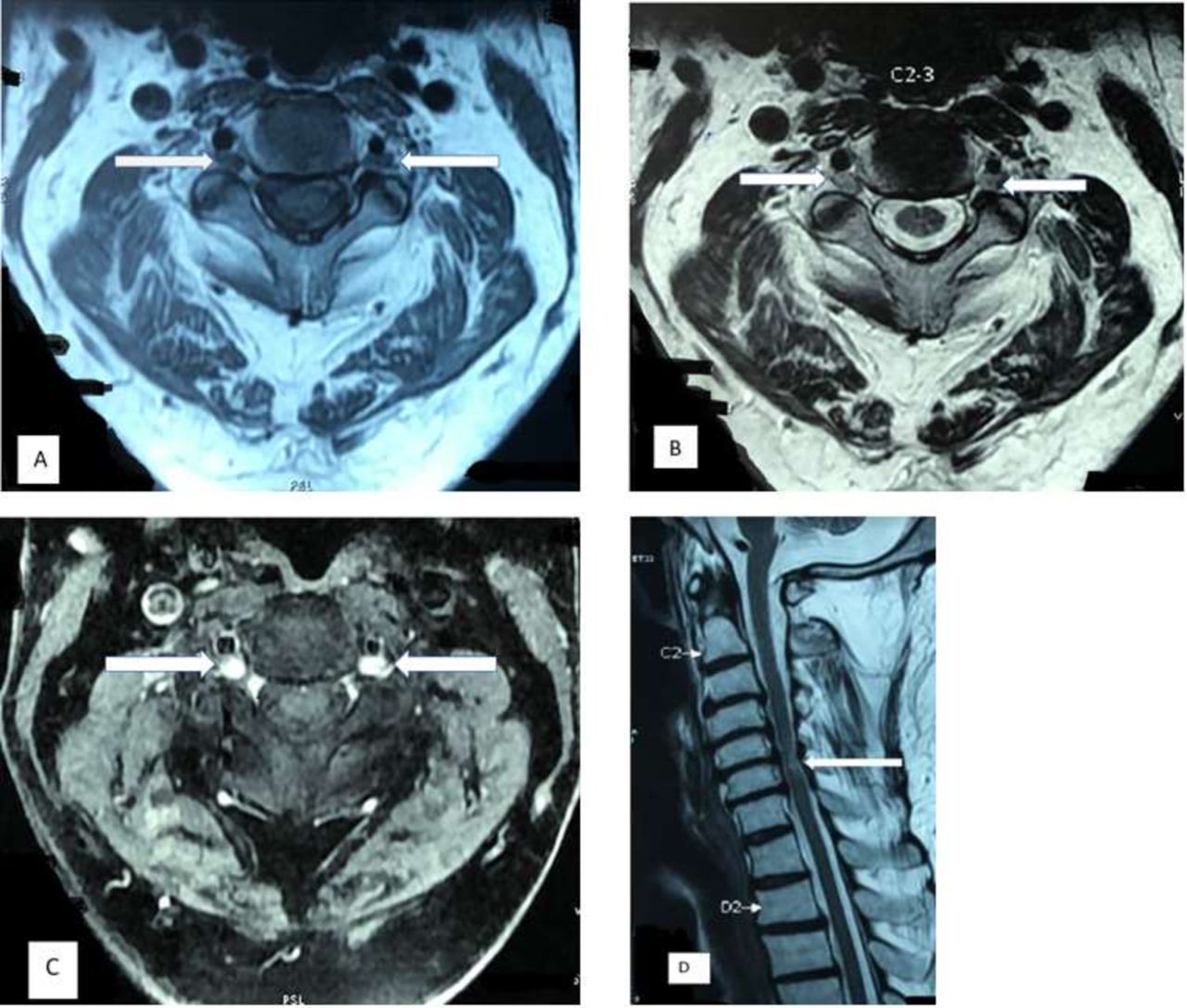
MRI of the cervical spine in axial plane showing T1-weighted hypointense (A) and T2-weighted hyperintense (B) with T1-weighted Short Tau Inversion Recovery (STIR) post contrast enhancing (C) lesions at the C2–C3 vertebral level suggestive of dorsal root ganglionitis (arrows). (D) MRI in sagittal plane showing the T2-weighted hyperintense lesion in the spinal cord at the level of C6 vertebra suggestive of myelitis (arrow).
{kind=link}
{kind=link}
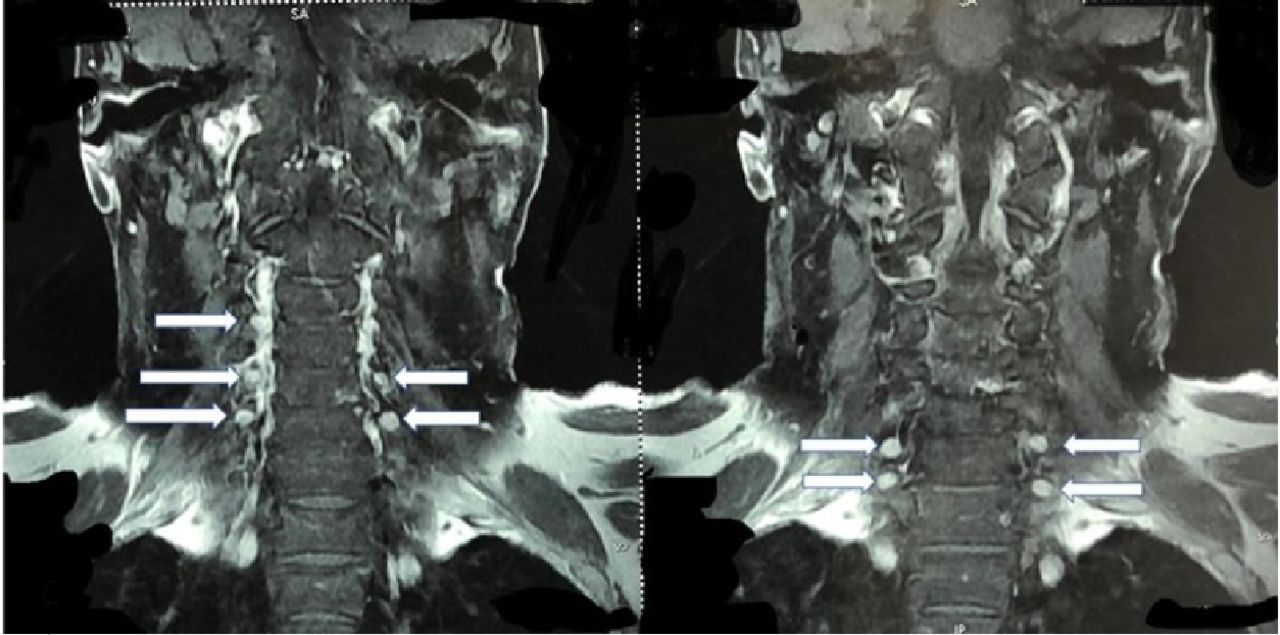
MRI of the cervical spine in coronal plane showing T1-weighted STIR post contrast-enhancing enlarged cervical dorsal root ganglion involvement at multiple levels suggestive of ganglionitis (arrows).
The mixed upper and lower motor neuron signs in our patient are explained by the coexistence of cervical cord myelitis, peripheral neuropathy and ganglionitis. Leprosy mainly presents with exteroceptive sensory loss as either mononeuropathy or mononeuritis multiplex. In a few patients, the kinesthetic sensory loss can occur due to dorsal root ganglion involvement resulting in pan-sensory loss.1 There are only a few reported cases of confirmed leprosy presenting with ganglionitis and myelitis. The presence of ganglionitis suggests an inflammatory response to bacteria even in the absence of its direct invasion2 3 and thus requires immunosuppression with steroids and multidrug therapy for leprosy. Our patient had significant clinical improvement with treatment similar to the earlier case report.4
Learning points
Hansen’s disease involves exteroceptive sensory loss. It can present with myriad neurological manifestations with mixed upper and lower motor neurological signs.
Presence of proximal kinesthetic sensory loss suggest dorsal root ganglion involvement.
Management requires glucocorticoids and multidrug therapy for leprosy.
Footnotes
Twitter @RasmiKGMU
Contributors PB, RRS, MM and AW were involved in patient management and data collection. PB prepared the manuscript. All the authors have critically revised the manuscript and responsible for intellectual content of the final draft.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.