Article Text

Statistics from Altmetric.com
Description
A 63-year-old woman presented with diplopia and left upper-lid ptosis. Ophthalmological assessment showed occulomotor nerve palsy and low vision in the left eye. Brain MRI showed a signal corresponding to a cystic lesion in the left anterior clinoid process (ACP) with a hyperintense signal on T2-weighted images, an intermediate signal on diffusion-weighted images, and no supression of the T1-hyperintense signal on fat saturated images. There was no fluid correction in her paranasal sinus(figure 1).

Preoperative CT/MRIs. (A) Axial T1-weighted images showing an anterior clinoidal mucocele (arrow). (B) Axial T2-weighted images showing an anterior clinoidal mucocele (arrow). (C) Coronal T2-weighted image showing that the left optic nerve (arrow head) exists more medially than the mucocele (arrow). (D) Coronal CT suggesting that the mucocele dissolves the anterior clinoidal process and optic strut (arrow). There are onodi cells bilaterally (square).
In a little while, the patient’s symptoms improved; thus, outpatient follow-up was conducted at our department. However, 6 months later, she presented with acute loss of vision for 1 week; brain MRI showed a cystic lesion with definite growth in the left ACP.
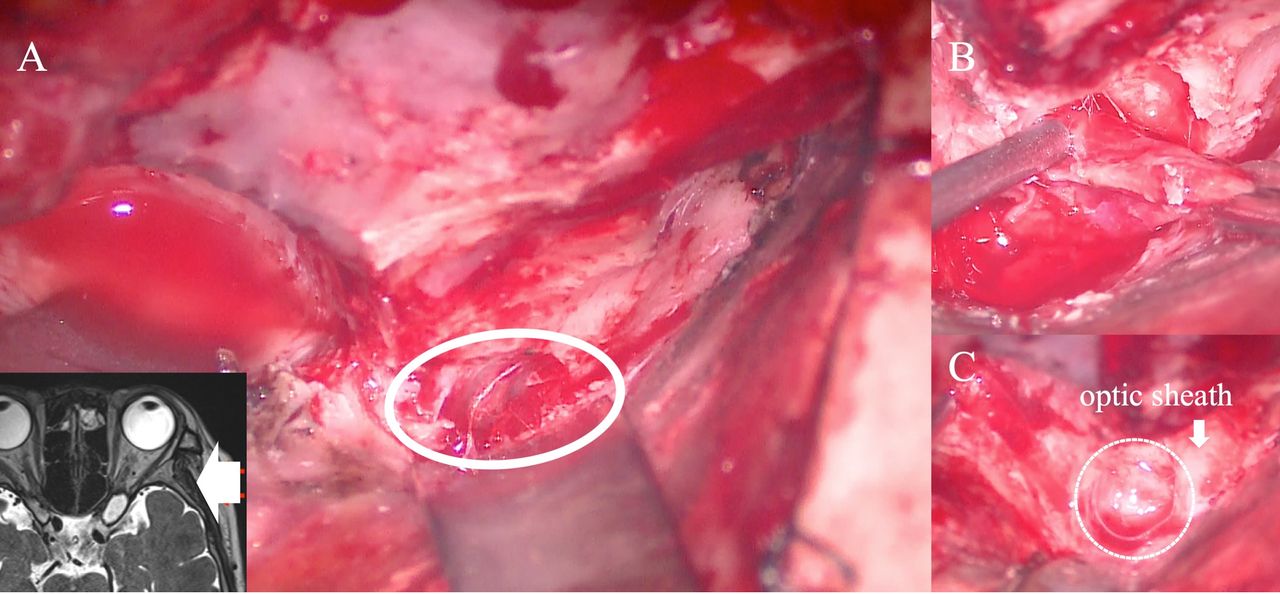
The patient underwent surgery, where a left pterional craniotomy was performed. The ACP was drilled away through an extradural approach, allowing for the exposure of the mucocele. Thereafter, the mucocele was resected, and the roof of the optic nerve canal was drilled, decompressing the optic nerve (figure 2). The postoperative pathological results suggested inflammation of the nasal mucosa.

{kind=link}
{kind=link}
Operative field view (from the direction of the arrow). (A) After the left pterional craniotomy, the mucocele was exposed (circle) through an extradural approach. (B) The mucous membrane is held with forceps. (C) Operative field after removing the mucous membrane. Dot circle indicates the anterior clinoid process space.
The patient’s visual acuity recovered remarkably at 1 month postoperation.
The rate of ACP pneumatisation is around 9.5%. Pneumatised patterns are classified according to the route of pneumatisation, that is via the optic strut, the anterior root, or both.1 Awareness of these variations in pneumatisation can prevent the destruction of the mucous membrane and the occurrence of surgical complications, such as cerebrospinal fluid leakage, following an anterior clinoidectomy.
Blockage of the drainage of the paranasal sinus for any reason can result in the accumulation of trapped secretions and mucocele. Owing to the proximity of the ACP to the optic nerve, patients with mucocele in this location often present with ocular symptoms.2
Prompt surgical treatment is usually advocated to achieve best recovery.3 Surgical options include open surgical resection or transnasal endoscopic approach. The latter may be preferable to the cases where sinus cysts expand to the ACP. Nonetheless, if the mucocele is localised in the ACP, cystic resection by craniotomy may be safer, because the cystic area is over the optic nerve by transnasal endoscopic surgery. However, a history of sinusitis can aid in the diagnosis of a reversible form of optic neuritis, for which proper medical treatment with steroids and antibiotics may be preferable to surgical intervention.2
Learning points
Awareness of anterior clinoid process (ACP) pneumatisation can prevent the occurrence of cerebrospinal fluid leakage as a result of an anterior clinoidectomy.
Patients with anterior clinoid mucocele presenting with visual loss who have a history of sinusitis receive only medical treatment with antibiotics and can thus avoid surgery.
An endoscopic approach may be preferable to cases where the sinus cysts expand to the ACP. However, if the mucocele localized in the ACP, the cystic resection by craniotomy or endoscopic trans-orbital approach may be safer, because the cystic area is over the optic nerve by transnasal endoscopic surgery.
Footnotes
Twitter @KAZ
Contributors KK drafted the manuscript. KO supervised the manuscript. SO edited the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.