Article Text

Statistics from Altmetric.com
Description
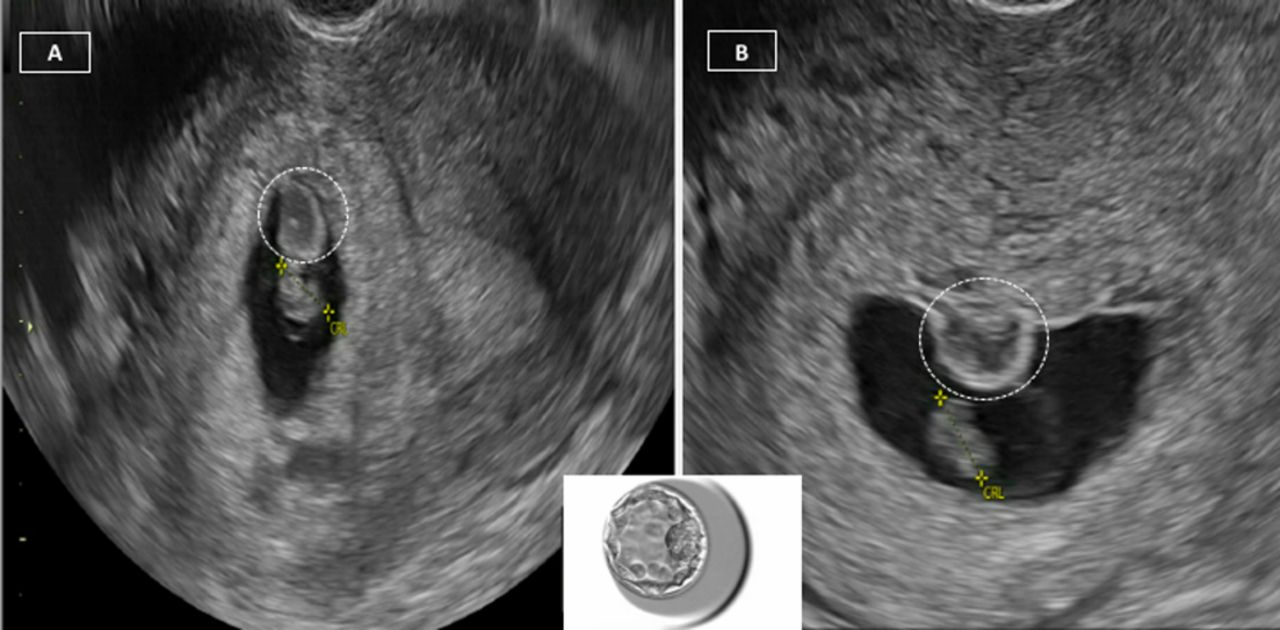
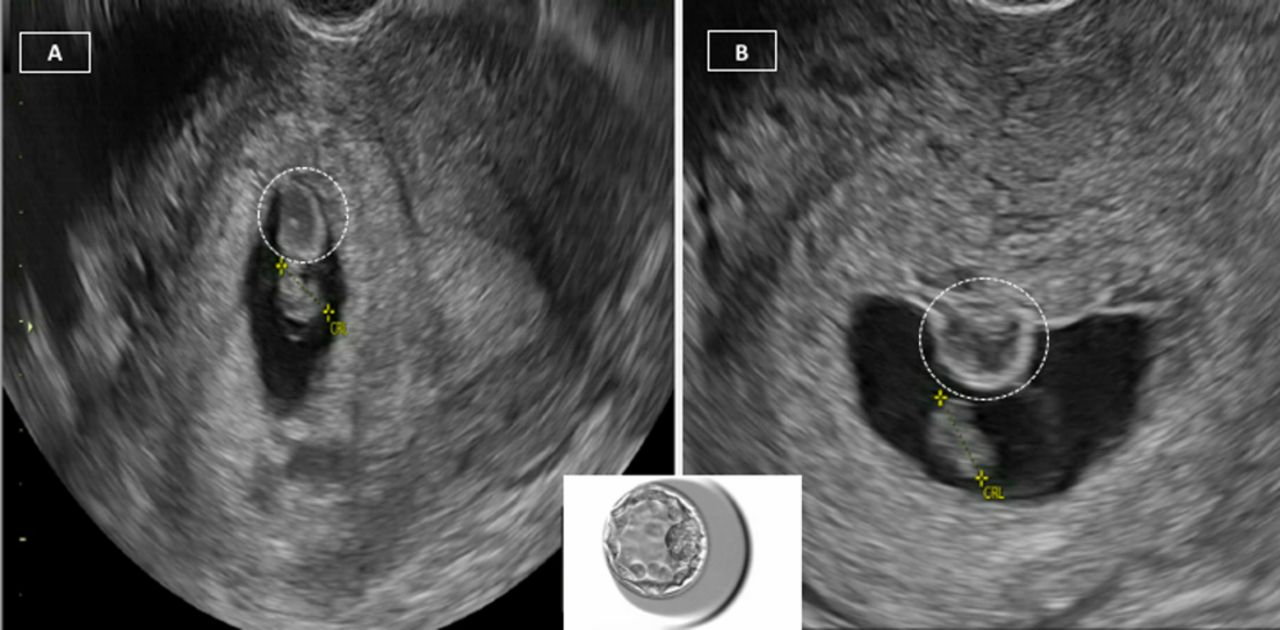
A 39-year-old nulliparous woman with a 1 year history of involuntary infertility underwent in vitro fertilisation and fresh single blastocyst transfer (figure 1, inset). Transvaginal ultrasonography on cycle day 51 showed a single intrauterine gestational sac with fetal pole. The crown-rump length measurement was 8.51 mm (6 weeks and 6 days), with a cardiac cavity of 114 beats/min (figure 1A, Panel A). A 7.0×7.8 mm mass extending from the choriodecidual surface was noted superior to the fetal pole (figure 1A, Panel A). A second transvaginal ultrasonogram was performed 2 weeks later. This ultrasonogram showed an enlarged yolk sac, minimal interval growth of the fetal pole and absent cardiac activity. The previously visualised mass was still present and measured 10.7×8.3 mm (figure 1B, Panel B). A missed abortion with an incidental chorionic bump (CB) was diagnosed. The patient was treated with misoprostol. Cytogenetic analysis of products of conception could not be performed due to the absence of viable chorionic villi. Her transvaginal ultrasonogram 4 weeks later was unremarkable.
{kind=link}
(A) Transvaginal ultrasonography at cycle day 51 showing a single intrauterine foetal pole (yellow calliper) and chorionic bump (dotted white circle); (B) transvaginal ultrasonography 2 weeks later showing minimal interval growth of the foetal pole (yellow calliper) and persistent chorionic bump (dotted white circle); inset—single blastocyst that was transferred.
A CB is defined as a convex bulge from the choriodecidual surface into the first‐trimester gestational sac.1 The prevalence of CB ranges between 0.4% and 0.7%.2 3 The aetiology of CB remains unknown. However, it is thought that the increased bleeding tendency in the decidual shell caused by the developing placenta plays a role in the formation of the CB.4 5 This haematoma that forms in the intervillous space of the chorionic layer can extend or bulge into the gestational sac in an oval or crescent form.4 5 Histopathological analysis of CB usually reveals haematoma remnants and villous structures consisting of cytotrophoblast and syncytiotrophoblast.4
The association between CB and poor pregnancy outcome remains controversial. In one study of 1900 first trimester pregnancy ultrasonograms, eight cases of CB were detected, of which five had live births and the remaining three experienced miscarriages.2 In another study of 3375 pregnancies, CB was diagnosed in 23 cases.3 All pregnancies resulted in a live birth, except for one pregnancy affected by trisomy 21. In contrast, a case–control study comparing the outcomes of 52 CB cases with 151 controls reported double the risk of miscarriage in the CB group.6 A systematic review of CB in pregnancy concluded that CB is a risk factor for non-viability in pregnancy; however, if the pregnancy is otherwise normal, then most result in a live birth.1 Studies have also suggested that CB seen during the first trimester should be followed with serial ultrasonogram examinations into the second trimester.4 5 CBs that resolve by the second trimester do not seem to increase antenatal or perinatal complications.5 In the context of the current case, we speculate that the pregnancy was likely chromosomally abnormal, given the presence of an enlarged yolk sac and the absence of cardiac activity, though cytogenetic analysis would have been beneficial.
Patient’s perspective
My case demonstrates the rare finding of chorionic bump.
Learning points
A chorionic bump (CB) is defined as a convex bulge from the choriodecidual surface into the first‐trimester gestational sac.
The impact of CB on pregnancy outcome is controversial.
A systematic review has suggested that CB is a risk factor for non-viability in pregnancy; however, if the pregnancy is otherwise normal, then most result in a live birth despite the CB.
Footnotes
Contributors KMC, SW and NS involved in the manuscript preparation and literature search. NP contributed in clinical imaging, manuscript preparation and literature search.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.