Article Text

Statistics from Altmetric.com
Description
A 53-year-old postmenopausal woman with non-alcoholic steatohepatitis cirrhosis, type II diabetes mellitus, hirsutism, depression and morbid obesity was evaluated for new onset seizures prior to liver transplant. The patient had been admitted with repeated bouts of hepatic encephalopathy over the past several months. During her current admission, she had an episode suggestive of a seizure and it was thought to be related to concomitant severe hypoglycaemia. Patient denied having a prior history of seizures or any episode of unexplained loss of consciousness. She also denied any traumatic brain injury or family history of epilepsy.
Physical examination revealed an obese woman, in no apparent distress with hypo-phonetic heart sounds and lungs clear to auscultation bilaterally. Abdominal examination was unremarkable, and extremities showed no oedema or rash. Her neurological examination evidenced preserved cranial nerves, no papilledema, unaltered extraocular muscle movements with normal facial motor and sensory functions. Patient had preserved sensation throughout as well as motor strength, with brisk reflexes, yet no Babinski or Hoffman noted. Cerebellum evaluation revealed a bilateral, hand predominant, intentional tremor.
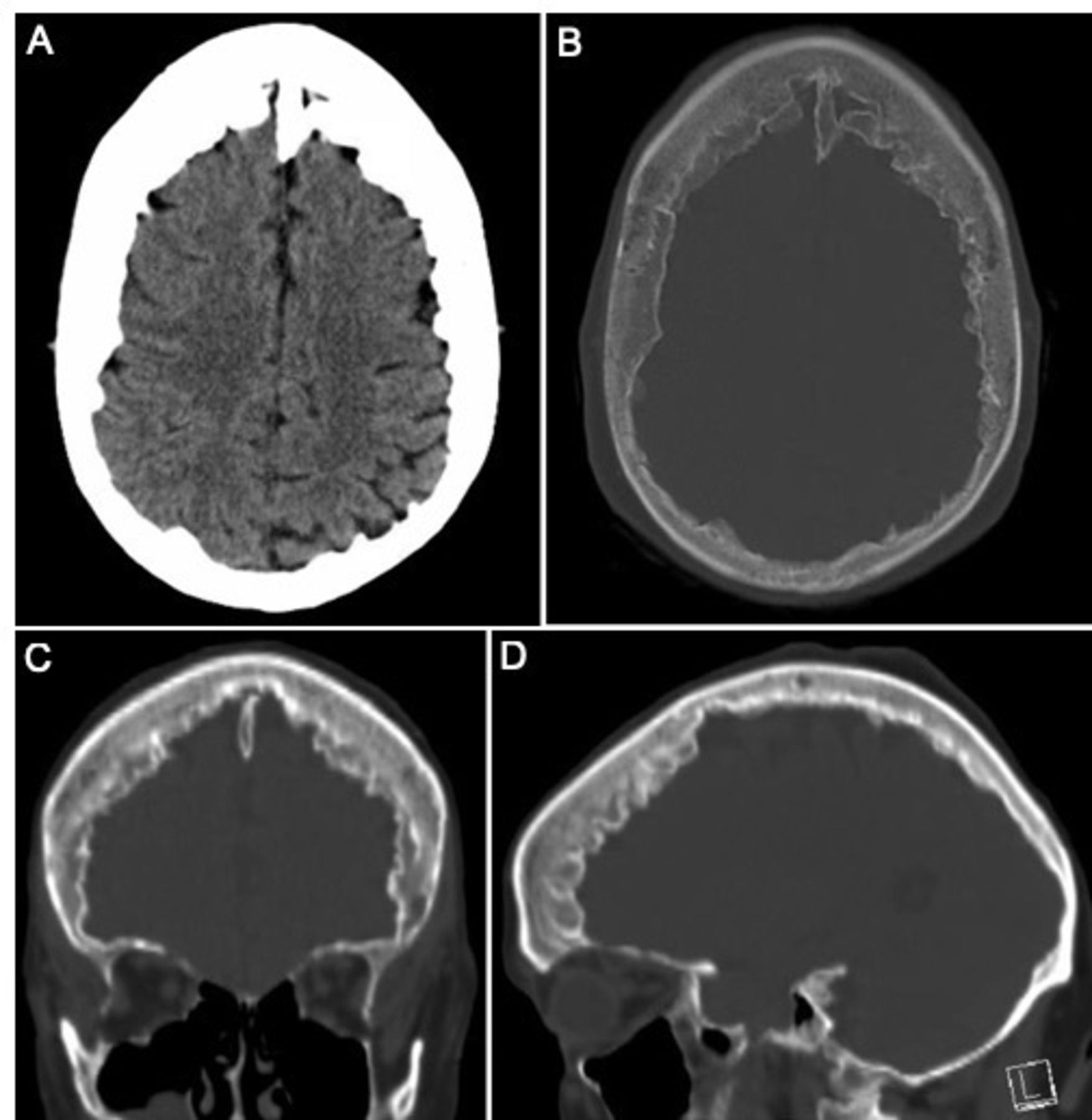
For her seizure work up, a routine electroencephalogram was obtained which was unremarkable and without any epileptiform features. Her non-contrast CT head (figure 1) revealed no intracranial haemorrhage, midline shift or mass effect, with mild chronic microvascular ischaemic changes of the periventricular and subcortical white matter. However, her CT scan was notable for hyperostosis frontalis interna. We attributed her seizure to the concomitant severe hypoglycaemic and refrained from starting any antiepileptic medication.
{kind=link}
CT head with hyperostosis frontalis interna: (A, B) axial, (C) coronal and (D) sagittal non-contrast CT head (bone window), showing continuous thickening of the frontal bone.
As an incidental finding, this patient presented with a type D hyperostosis frontalis interna (HFI) with >50% of continuous overgrowth of the frontal bone. HFI is nine times more frequent in women and when present along with virilisation, obesity and neuropsychiatric disorders is known as Morgagni-Stewart-Morel syndrome.1 Frontal bone thickening is mainly of the endocranium, leaving the cortical bone and periosteum unaffected. It has also been described in association with chronic headaches and rarely with seizures.2 This incidental image finding should not alarm neurologists yet should raise awareness about a possible susceptibility for headaches and seizures as part of the syndrome described above.
Learning points
Hyperostosis frontalis interna (HFI) is a continuous overgrowth of the frontal bone and has been described in association with chronic headaches and rarely with seizures.
HFI is nine times more frequent in women and when present along with virilisation, obesity and neuropsychiatric disorders is known as the Morgagni-Stewart-Morel syndrome.
Footnotes
Twitter @Gabriel07052207
Contributors All authors have contributed to and agreed on the content of the manuscript. The respective roles of each author are as follows: GT-A conceptualised the report and made substantial contributions to the design, drafting and revision of the work. JM significantly contributed to drafting and critically reviewing the paper. All authors approved the final version of the manuscript and assume accountability for all aspects of the work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.