Article Text

Statistics from Altmetric.com
Description
A 38-year-old man presented with fever, shortness of breath, dyspnoea on exertion and myalgia for 1 week. He reported contact with a friend who had COVID-19 pneumonia approximately 3 weeks before his symptoms developed. At the emergency room, his temperature was 38.5°C whereas the pulse and respiratory rate were normal; however, his oxygen saturation on room air was 92%. Nasopharyngeal swab tested positive for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) on reverse-transcription polymerase chain reaction (RT-PCR).
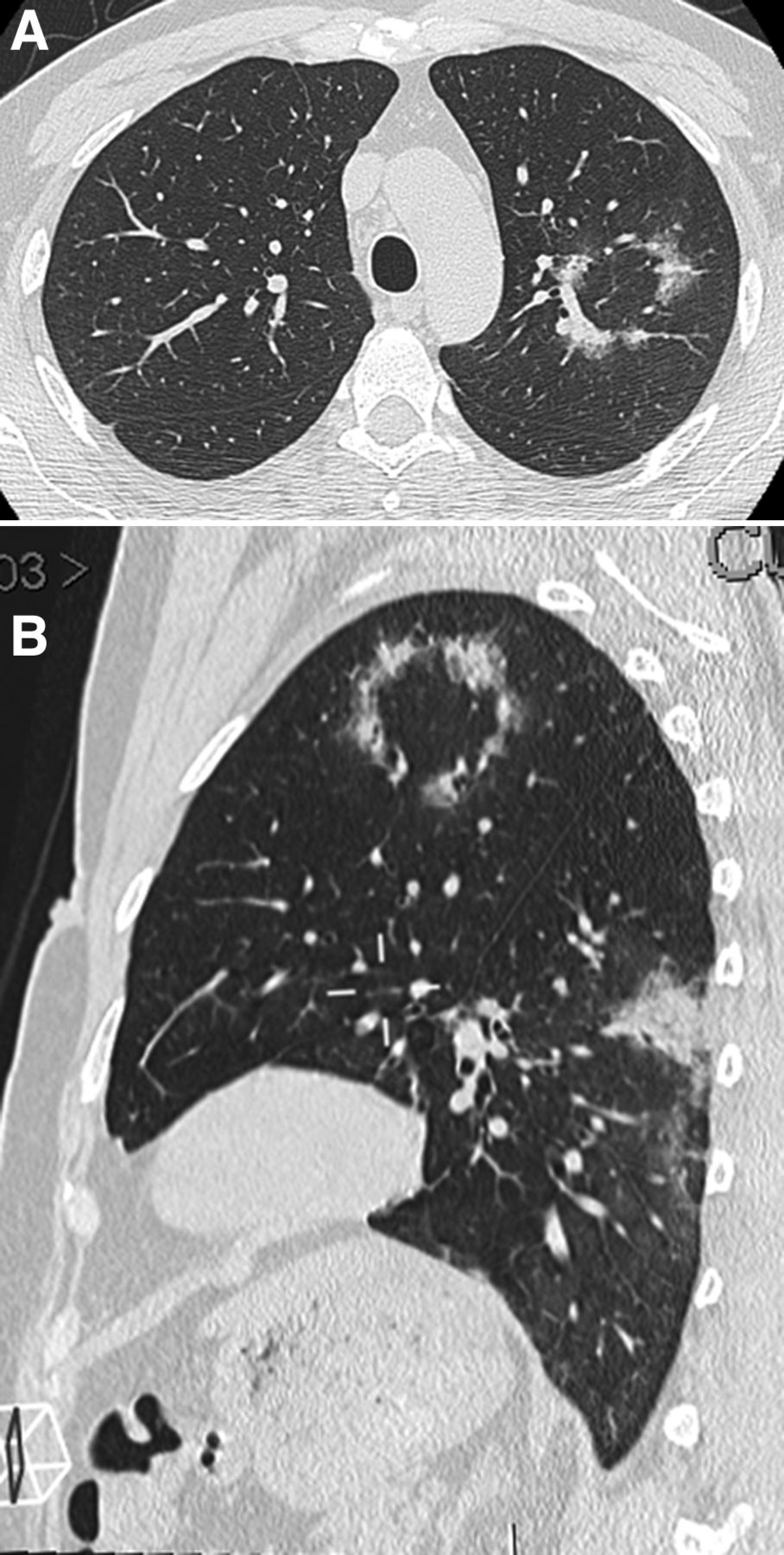
Chest CT performed on the seventh day of his illness revealed a ring-like opacity in the apicoposterior segment of the left upper lobe. This ring-like abnormality was a mixture of consolidation and ground-glass opacity along with the peribronchovascular bundle with wavy contour, mimicking a flame (figure 1A,B). Therefore, ‘ring of fire’ is proposed to describe this appearance. Minimal bronchiolectasis within the ring was also noted. Several other foci of consolidation and ground-glass opacity were observed, scattered in both lungs but more on the left. There was neither pleural effusion nor significant enlarged mediastinal lymph nodes.
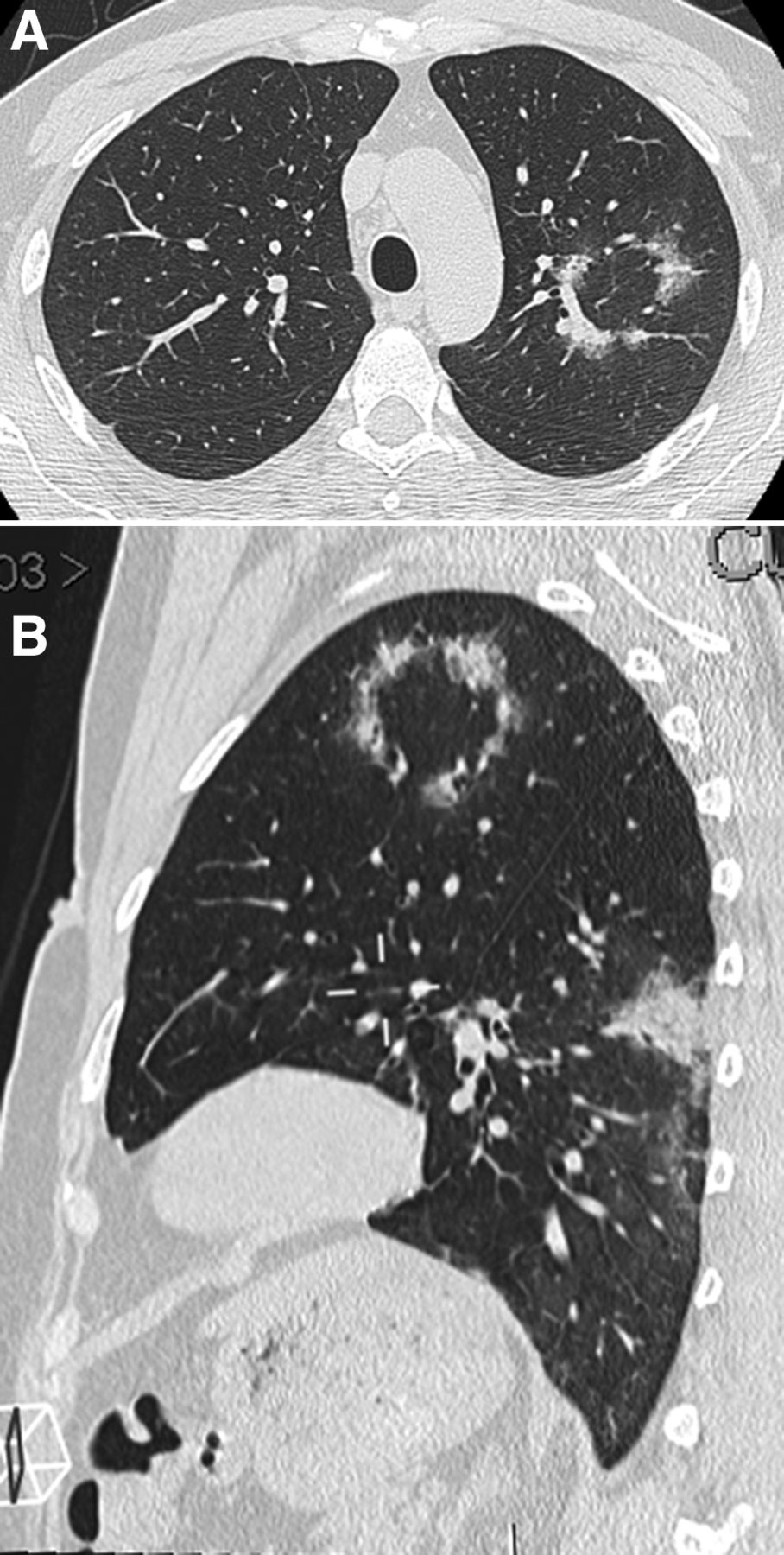
(A) Chest CT axial view: ring-like abnormality consisting of consolidation, ground-glass opacities and mild bronchiolectasis surrounding an area of the normal lung in the apicoposterior segment of the left upper lobe, creating the ‘ring of fire’ appearance. (B) Chest CT sagittal oblique view: consolidation along with the peribronchovascular bundles in the left upper lobe forming a ‘ring of fire’.
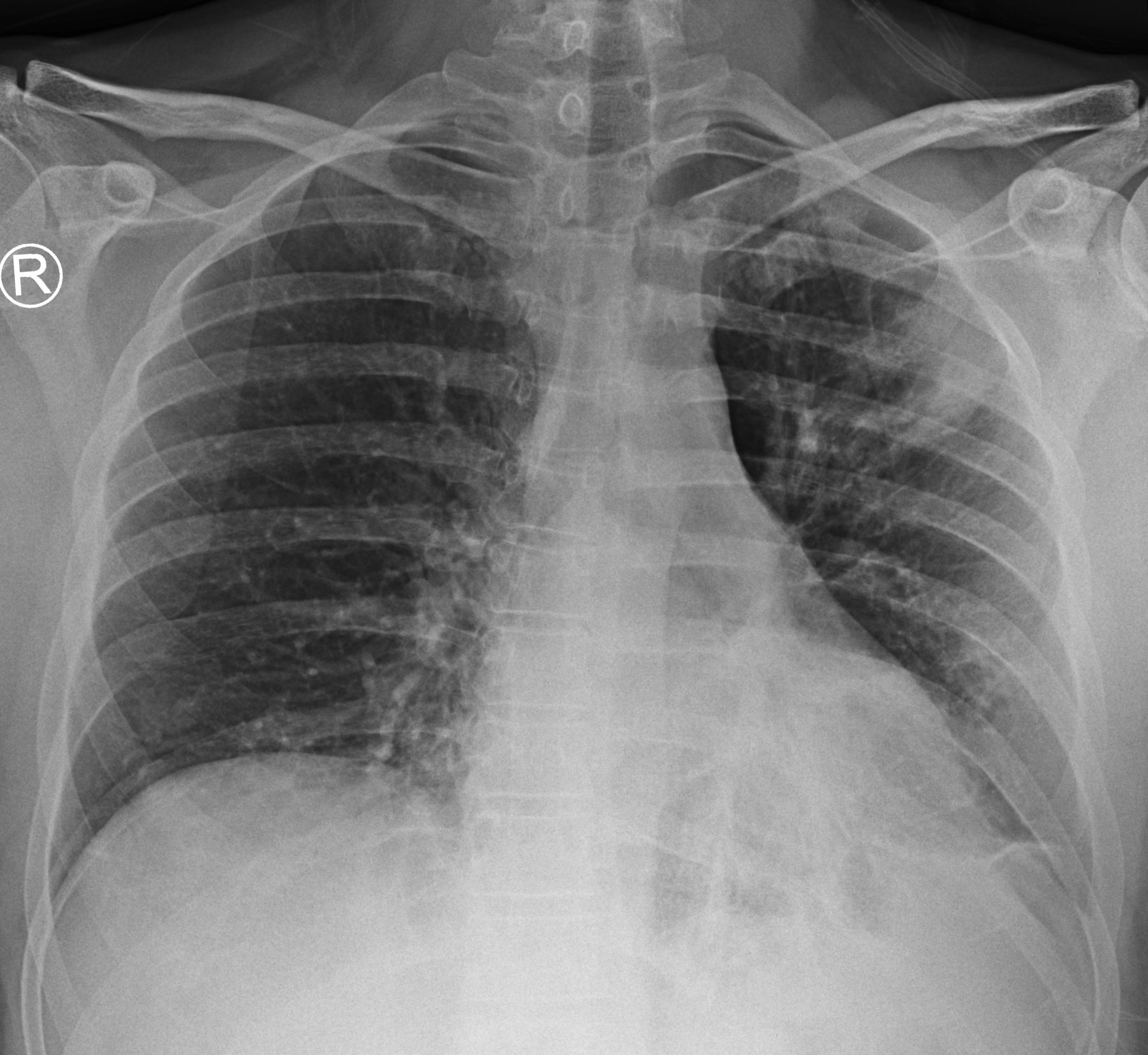
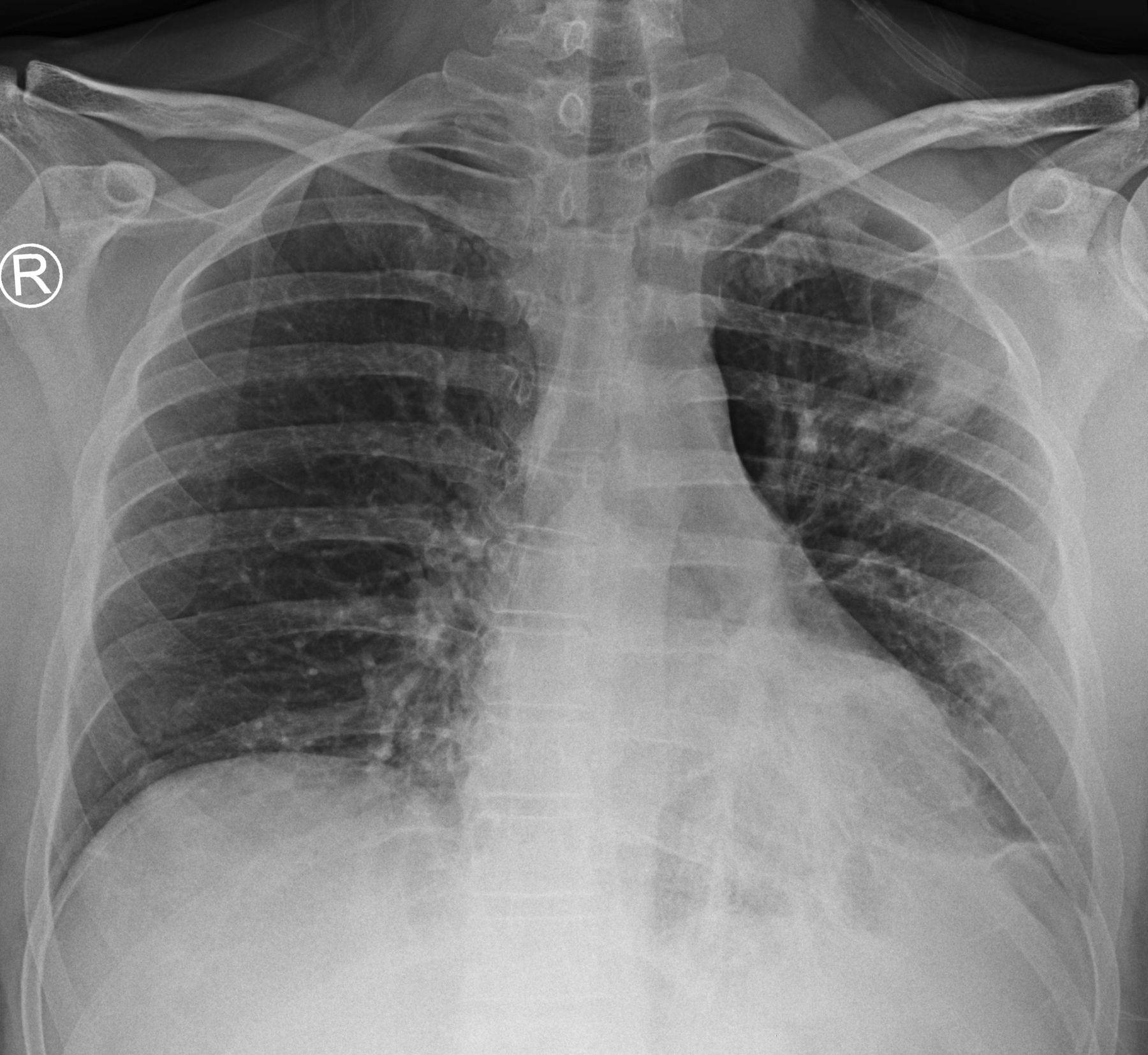
Chest X-ray obtained 1 day later, revealed a curvilinear band-like opacity in the left upper lung zone, mimicking a cavity-like appearance and corresponding to the ring of fire appearance in the prior chest CT (figure 2). Consolidation along bronchi in the left retrocardiac region was also present.
{kind=link}
{kind=link}
Chest X-ray: curvilinear band-like opacity in the left upper lung, creating pseudocavity. Peribronchovascular consolidation in the left lower lung zone is also noted.
The patient was admitted and treated with darunavir, ritonavir, favipiravir, hydroxychloroquine, azithromycin and ceftriaxone. His follow-up chest X-ray 1 week after the start of treatment was normal.
Since the beginning of the outbreak in December 2019, many radiologic findings in COVID-19 pneumonia have been described in the literature. The predominant lung finding is ground-glass opacities, some with a round morphology. A crazy-paving pattern, consolidation with or without a peripheral halo, air bronchograms, thickened interlobular septa and adjacent pleura are also reported.1–4 The abnormalities have a predilection for the peripheral and subpleural regions of the lungs and are commonly bilateral. A peribronchovascular distribution has not been common in the reports of COVID-19 pneumonia.4
A central ground-glass opacity surrounded by denser air-space consolidation in the shape of a crescent or a ring, so-called reverse halo sign or atoll sign,5 6 is also reported in COVID-19 pneumonia.7 8 In our case, unlike the atoll sign, the ring of fire has a radiologically normal lung in the centre, surrounded by a mixture of consolidation and ground-glass opacity. Bronchiolectasis within the ring shadows is also present. These ring shadows are composed of lung abnormalities along with peribronchovascular bundles.
Learning points
Chest CT and chest X-ray are critical parts of the radiologic evaluation of COVID-19.
Ring-shaped abnormality, consisting of consolidation, ground-glass opacities and bronchiolectasis surrounding normal lung, creating the ‘ring of fire’ appearance.
The ‘ring of fire’ may appear like a cavity on chest X-ray, and thus leads to misdiagnosis since COVID-19 is not associated with cavities.
Acknowledgments
The authors would like to thank the staff of Bumrungrad Research Center for their administrative help.
Footnotes
Twitter @Warawut
Contributors NP and KP conceived of the idea, provided patient care and drafted the manuscript. NP retrieved the patient data. WS and LP-B helped to edit the manuscript. All authors read and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.