Article Text

Statistics from Altmetric.com
Description
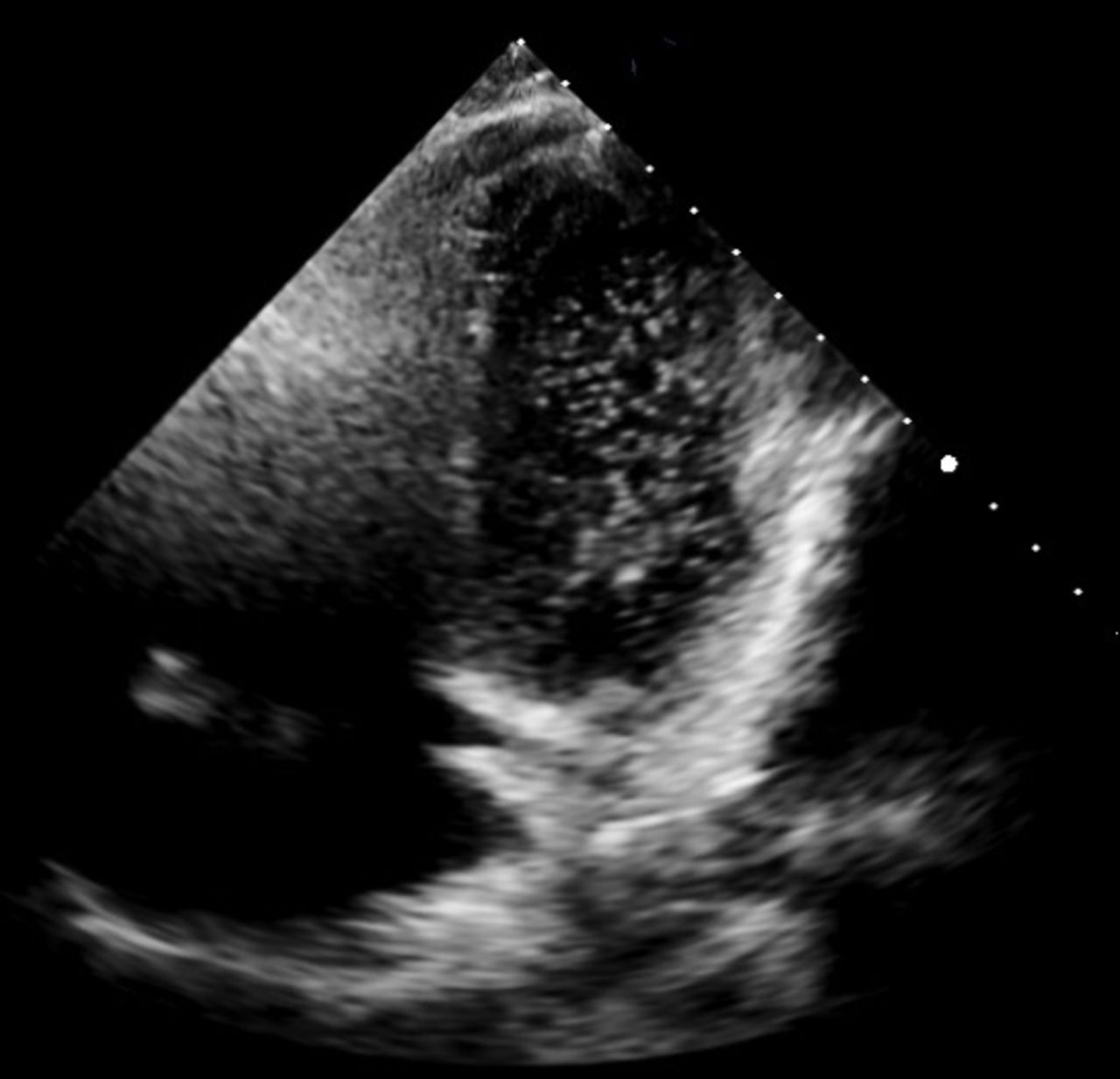
A 44-year-old male was admitted to the respiratory unit with a history of worsening dyspnoea, productive cough and fever. He was an active smoker with a background of Child-Pugh class A alcoholic cirrhosis and previous intravenous drug use. On admission, he was feverish, tachypnoeic and was requiring an FiO2 of 60% to maintain oxygen saturations >94%. Crepitations were heard throughout the right lung; cardiovascular and abdominal examinations were normal. Laboratory tests showed a neutrophilia (8.9×109/L), thrombocytopaenia (45×109/L), normal haemoglobin (130 g/L) and liver biochemistry. Arterial blood gas demonstrated hypoxaemia; PaO2 8.79 kPa on 60% oxygen and pCO2 5.44 kPa. CT pulmonary angiogram was negative for pulmonary embolism and demonstrated consolidation in the right lung in keeping with infection (figure 1). He was managed for severe community-acquired pneumonia. Despite 2 weeks of intravenous antibiotics and clinical resolution of pneumonia, he had ongoing dyspnoea on exertion and oxygen requirement. A repeat CT scan demonstrated improvement of the previously noted consolidation in the right lung. A two-dimensional transthoracic echocardiogram (TTE) revealed mildly reduced left ventricular function and no intracardiac shunts. Contrast-enhanced TTE using peripheral injection of agitated colloid solution showed multiple microbubbles in the left ventricle, appearing after the third cardiac cycle, suggestive of an intrapulmonary shunt (figure 2); confirming the suspected diagnosis of hepatopulmonary syndrome (HPS).

CT chest performed on admission demonstrating extensive consolidation throughout the right lung consistent with community-acquired pneumonia.

{kind=link}
{kind=link}
Contrast-enhanced two-dimensional transthoracic echocardiogram demonstrating multiple microbubbles in the left ventricle. The presence of microbubbles in the left heart occurred ≥3 cardiac cycles after right heart appearance, thus, excluding intra-atrial shunting.
Following risk assessment, the patient was deemed unsuitable for long-term oxygen therapy (LTOT) as both he and his partner were active smokers and smoking cessation was deemed unlikely. He was discharged 1 month following admission after being weaned off oxygen and PaO2 was 7.6 kPa on room air. At follow-up, his hypoxaemia was persisting (PaO2 7.4 kPa), but despite this, his dyspnoea had improved. Spirometry was consistent with a smoking history, with a forced expiratory volume in 1 s (FEV1) 51% of predicted, forced vital capacity (FVC) 77% of predicted and FEV1/FVC ratio of 67%. The patient has committed to smoking cessation and is being considered for both LTOT and liver transplantation.
HPS is as a triad of liver disease, evidence of intrapulmonary vascular dilatations and pulmonary gas exchange abnormalities leading to arterial deoxygenation.1 When evaluating the hypoxaemic cirrhotic patient consideration of common pathologies including infection, chronic obstructive pulmonary disease, cardiac failure, ascites and anaemia is essential. In this case, the degree of hypoxaemia and its persistence despite resolution of infection prompted further evaluation and identification of HPS. Platypnoea and orthodeoxia are suggestive, but not pathognomonic, features of HPS and were not assessed in our patient.2 Our patient likely had compensated chronic hypoxaemia prior to presentation which was significantly exacerbated by infection. HPS often presents insidiously and may be precipitated by mild liver disease; therefore, a high suspicion of index is essential.2 LTOT is a recommended supportive measure in HPS.1–3 However, as in this case, contraindications to LTOT may be present; careful risk-benefit assessment must be undertaken. Liver transplantation is the only effective known treatment option with significant improvement in hypoxaemia in the majority of patients.2 3
Learning points
Hepatopulmonary syndrome (HPS) should be considered in all patients with known liver disease and unexplained hypoxaemia.
Management options in HPS are limited; long-term oxygen therapy (LTOT) is beneficial. Liver transplantation remains the treatment of choice for HPS with complete resolution expected. Severe hypoxaemia due to HPS (PaO2 <8.0 kPa) warrants a higher priority for transplantation.
Ongoing cigarette smoking is a contraindication to both LTOT and liver transplantation.
Footnotes
Contributors MO and SM wrote up the case details and performed the literature search. SA was involved in clinical case management and evaluated the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.