Article Text

Statistics from Altmetric.com
Description
Haemangiomas generally occur in 5%–10% of children less than 1 year with endothelial cell proliferation, a rapid growth phase, and is considered to be the most common tumour in childhood.1 An additional neoplastic variant appears in older people or in midlife.2 The uvula, hard palate and the soft palate are rarely affected.3 The occurrence of the haemangioma on the palatal mucosa is extremely rare.4
The retention of a complete denture is greatly influenced by posterior palatal seal area which forms the junction of the hard and soft palate. The present case is of importance due to the presence of a palatal tori extending onto the soft palate with a haemangioma on its posterior-lateral aspect. This makes it challenging to achieve the posterior palatal seal while fabricating complete dentures.
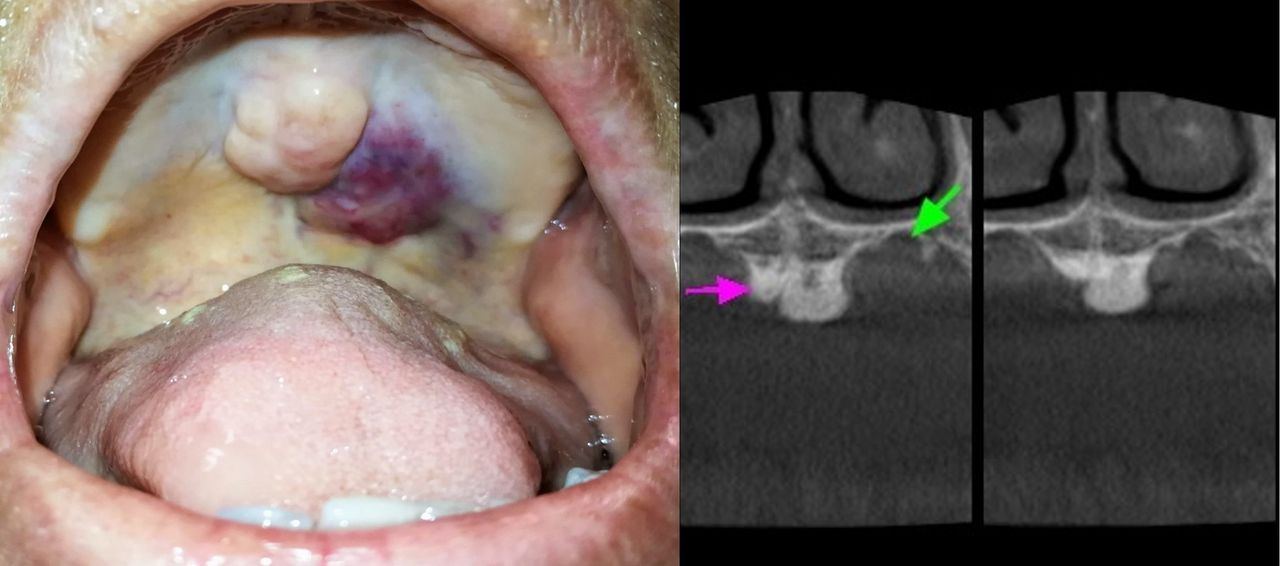
A 63-year-old woman presented with problem of a growth in her palate. She reported that this growth had been present for approximately 1 year, was asymptomatic and had not changed in size. There was no history of pain, pus discharge or bleeding, or any other secondary symptoms. She did not have any significant medical history. Intraoral examination revealed an edentulous maxillary arch and a mid-palatal torus measuring approximately 2×2 cm with a well-defined border and pebbly surface in the centre of the hard palate. A pinkish growth was present on the left posterolateral part of the hard palate just 2 cm lateral to the midline in an area between the maxillary first and second molars, measuring approximately 2×1.5 cm in diameter (figure 1). On palpation, it was soft in consistency, non-tender and compressible but not pulsatile or reducible. Based on these clinical findings, a provisional diagnosis of capillary haemangioma and differential diagnosis of arteriovenous malformation were made.

Intraoral view of palatal tori with haemangioma posteriolaterally and cone beam CT (CBCT) image of the same. Coronal section in mid-palatal region showing resorption of palatal bone (green arrow) on the left side. Note the tori in the centre of the palate (pink arrow). (Scale 1.43) Planmeca 3Ds CBCT unit (Helsinki, Finland); 200 μm voxel, 90 kVp, 12 mA, 12.35 s exposure.
Cone beam CT (CBCT) was advised to rule out any pathological changes of the palatal bone.
Axial, coronal and sagittal sections were obtained, which revealed a lobulated mass with the density of bone tissue that caused bulging in the centre of the hard palate confirming the presence of a palatal tori (figure 1, pink arrow). CBCT further showed thinning of bone at the posterior palatal area on the left side (figure 1, green arrow), suggestive of extension of the vascular lesion.
The patient was advised angiography to rectify the feeder vessel and block the same. Sclerosing injections like sodium morrhuate were also suggested.
However, the patient was reluctant for any investigations and opted for a non-invasive treatment.
Fabrication of a complete denture avoiding the tori and haemangioma was planned. Primary impressions were made with irreversible hydrocolloid. Border moulding with low fusing compound was done around the borders of the denture base around the tori and the haemangioma to create a bead line for retention. A complete denture with a U-shaped palatal plate was delivered to avoid the tori and any impingement onto the haemangioma (figure 2).

{kind=link}
{kind=link}
Intraoral view of U-shaped prosthesis avoiding the torus and haemangioma.
A 6-month follow-up showed no significant changes and good patient satisfaction.
Learning points
Haemangiomas are congenital hamartomas and vascular malformations which rarely present in the palate.4
Whenever vascular lesions are suspected, invasive investigations such as biopsy or aspiration should not be attempted.
The success of the denture generally depends on the design of the prosthesis. Here, anterior undercuts were engaged to gain retention. Palatal beading on the peripheral borders as well as around the tori helped to achieve an acceptable border seal without encroaching onto the haemangioma.
This design was practically feasible without the need for surgical intervention providing better aesthetics. The problem of lesser retention compared with a traditional complete denture was conveniently overcome by utilisation of labial undercuts.
Footnotes
Contributors AM: preparation of manuscript and photographs. PE: prosthetic treatment of case and preparation of manuscript. SKN: diagnosis and radiographic interpretation. KK: prosthetic treatment of case and photographs.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.