Article Text

Abstract
COVID-19 is a novel viral infection caused by severe acute respiratory syndrome-coronavirus-2 virus, first identified in Wuhan, China in December 2019. COVID-19 has spread rapidly and is now considered a global pandemic. We present a case of a patient with minimal respiratory symptoms but prominent bilateral groundglass opacities in a ‘crazy paving’ pattern on chest CT imaging and a negative initial infectious workup. However, given persistent dyspnoea and labs suggestive of COVID-19 infection, the patient remained hospitalised for further monitoring. Forty-eight hours after initial testing, the PCR test was repeated and returned positive for COVID-19. This case illustrates the importance of clinical vigilance to retest patients for COVID-19, particularly in the absence of another compelling aetiology. As COVID-19 testing improves to rapidly generate results, selective retesting of patients may uncover additional COVID-19 cases and strengthen measures to minimise the spread of COVID-19.
- respiratory system
- pneumonia (respiratory medicine)
This article is made freely available for use in accordance with BMJ's website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
Background
In December 2019, a novel virus, severe acute respiratory syndrome-coronavirus-2 (SARS-CoV-2), was identified in Wuhan, China. Initially thought to be comparable to influenza, our understanding of COVID-19, caused by SARS-CoV-2 is evolving daily. It has caused a global disturbance due to its high transmission rate. WHO officially labelled COVID-19 as a pandemic on 11 March 2020, with the disease having spread to >190 countries. As of 07 April 2020, there were more than 1 400 000 confirmed cases with over 80 000 deaths.1
SARS-CoV-2 is a non-segmented, positive sense RNA virus that was first isolated from people who had visited the Huanan seafood market in Wuhan, China.2 Coronaviruses are naturally found in bats, which were postulated to be the primary reservoir for zoonotic transmission to humans in prior cases of coronavirus infection.3 4 This is, expectedly also true for SARS-CoV-2 as genetic studies have identified more than 96% similarity in the whole genome sequencing of SARS-CoV-2 and a bat SARS-related coronavirus (RaTG13) in China.5 In addition, pangolins have also been identified as potential reservoirs of coronavirus.6 SARS-CoV-2 binds the ACE2 receptor located on type II alveolar cells and intestinal epithelia. This is the same receptor used by the severe acute respiratory syndrome coronavirus-1 (SARS-CoV-1), hence the technical name for COVID-19 being SARS-CoV-2.7 8
The clinical presentation for SARS-CoV-2 varies from being asymptomatic to developing mild upper respiratory tract infection to severe pneumonia resulting in acute respiratory distress syndrome.9 This has posed challenges in halting the transmission via droplets due to asymptomatic carriers as well as identifying patients who can potentially decompensate later in the clinical course. As we learn more about COVID-19, we need to adapt and identify the means of early diagnosis, its management and most importantly, its prevention. We present a case of an 80-ear-old man who posed a diagnostic dilemma and the thoughts behind our decision-making process which could be useful to other clinicians managing patients with COVID-19.
Case presentation
An 80-year-old man presented to the emergency department with dyspnoea and nausea. His comorbidities included atrial fibrillation requiring cardioversion currently receiving anticoagulation with apixaban, non-ischaemic cardiomyopathy causing biventricular heart failure and left bundle branch block requiring cardiac resynchronisation therapy-defibrillation placement with most recent ejection fraction of 54%, hyperlipidaemia, gastro-oesophageal reflux disease and pseudogout. He was a remote smoker having quit more than 50 years ago, worked as a financial planner and denied any concerning exposures. His dyspnoea was primarily with exertion and had gradually progressed over the preceding 6–8 weeks. His primary residence was in Tennessee but he travelled extensively for work, most recently to New York, almost 4 weeks prior to his presentation. He did not have any known sick contacts. In the week prior to presentation, the patient had an acute change in exertional dyspnoea that resulted in difficulty climbing a flight of stairs. This acute change correlated with new onset nausea and loss of appetite. Notably, he did not have fevers, cough, sputum production, haemoptysis, chest pain, orthopnoea, lower extremity oedema or weight gain. He initially sought recommendations from his local primary care provider a week prior to presentation who temporarily increased the patient’s dose of furosemide. However, this did not alleviate his dyspnoea.
Investigations
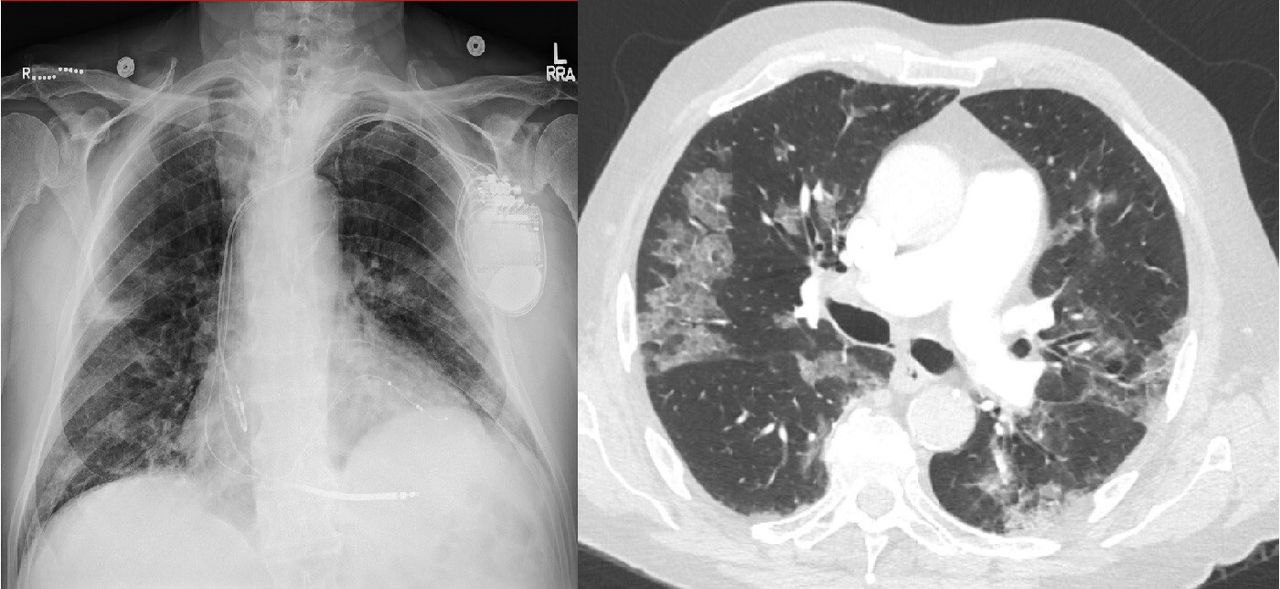
In the emergency department, he was afebrile and normotensive with mild tachypnoea and oxygen saturation of 92% on room air. On examination, he was well appearing, had bibasilar rales with a systolic murmur likely from known tricuspid regurgitation, but without significant jugular venous distension or lower extremity oedema. The remainder of his physical examination was unremarkable. Laboratory workup revealed normocytic anaemia with haemoglobin 119 g/L, normal white cell count of 7.5×109/L with reduced absolute lymphocyte count of 0.76×109/L, N-terminal pro brain natriuretic Peptide (NT-pro BNP) 1722 pg/mL (normal 5–128 pg/mL), D-dimer 1392 ng/mL (normal ≤500 ng/mL), C-reactive protein (CRP) 82.6 mg/dL (normal ≤8 mg/dL), high sensitive troponin T 26 ng/L (normal ≤15 ng/L) without significant change after 2 hours, aspartate aminotransferase 61 U/L (normal 8–48 U/L) with otherwise unremarkable liver function tests and a normal renal function panel. A 12-lead ECG showed a paced rhythm without significant changes from prior readings. Chest radiograph revealed new patchy airspace opacities bilaterally. Due to an elevated D-dimer and progressive dyspnoea, a chest CT scan with pulmonary angiogram was obtained. CT chest with pulmonary angiogram was negative for pulmonary embolism but demonstrated diffuse bilateral patchy groundglass opacities predominantly in the mid to lower lung zones, which were consistent with crazy paving pattern (figure 1). These findings were new compared with a scan obtained 12 months prior, which showed an unremarkable pulmonary parenchyma.
{kind=link}
Chest X-ray with bilateral patchy airspace opacities (left), CT chest with bilateral groundglass opacities and crazy-paving pattern.
He was admitted to the inpatient medicine service for further workup under modified contact and droplet isolation (use of gown, gloves, surgical mask and eye shield). Influenza and respiratory syncytial virus PCR were negative. Due to the COVID-19 pandemic, his travel history and reports of community transmission within the USA, a nasopharyngeal swab for SARS-CoV-2 PCR was obtained, which returned negative. The pulmonary medicine team was consulted for consideration of bronchoscopy for further diagnostic workup. Due to high suspicion of infection, haemodynamic stability and immunocompetent status, testing with an extended respiratory pathogen panel and repeat SARS-CoV-2 PCR was recommended. Both tests were negative 24 hours after the initial SARS-CoV-2 PCR. The case was reviewed with the institutional infection prevention and control team who recommended repeating SARS-CoV-2 PCR 48 hours from the initial test. This was subsequently obtained and was positive, consistent with COVID-19 infection. Importantly, due to high clinical suspicion, modified contract and droplet precautions were maintained while the SARS-CoV-2 PCR tests were pending.
Differential diagnosis
The differential diagnosis of his clinical presentation was broad and included viral or atypical infection including pneumocystis pneumonia, inflammatory/interstitial lung disease such as eosinophilic pneumonia, non-specific interstitial pneumonitis or hypersensitivity pneumonitis and heart failure exacerbation. Heart failure exacerbation was less likely due to a stable echocardiogram, normal cardiac device interrogation a week prior to presentation, stable weight and absence of volume overload on examination or imaging.
Treatment
The patient was subsequently transferred to a dedicated medicine service caring for patients positive for COVID-19. Due to reports of sudden acute decompensation in older patients with COVID-19,10 he was observed in the hospital for a longer duration despite being haemodynamically stable.
Outcome and follow-up
His inflammatory markers down-trended (table 1) which correlated with symptomatic improvement and he was discharged in stable condition after a total of 8 days of hospitalisation.
Laboratory parameters of patient admitted (day 0) with dyspnoea
Discussion
This case illustrates the importance of clinical suspicion and supplemental diagnostics including CT chest imaging and laboratory data to diagnose COVID-19. The primary symptoms in patients hospitalised with COVID-19 infection are fever (88.7%), cough (67.8%), fatigue (38.1%), dyspnoea (18.7%), myalgia (14.9%) and chills (11.5%). Nausea or vomiting (5.0%) and diarrhoea (3.8%) were less common. Common radiological findings included ground-glass opacities (56.4%) and bilateral patchy shadowing (51.8%). No radiological or CT findings were found in 17.9% of patients with non-severe disease and in 2.9% with severe disease. On admission, lymphocytopenia (83.2%), thrombocytopenia (36.2%) and leucopenia (33.7%) were noted. Elevations in serum CRP, D-dimer, creatine kinase, alanine aminotransferase and aspartate aminotransferase were reported in some cases.11
A recent study in China retrospectively reviewed the initial chest CT of patients with COVID-19 and found ground-glass opacity (61.3%) ground-glass opacity with consolidation (35.5%), crazy-paving pattern (25.8%), rounded opacities (25.8%) and air bronchograms (22.6%).12 ‘Crazy paving’ is a non-specific chest CT finding produced by the amplified density of lung parenchyma that manifests as a ground glass appearance superimposed on reticular thickening of the inter and intra-lobular septae.13 This can be seen in sarcoidosis, drug induced pneumonitis, pneumocystis jirovecii pneumonia, pulmonary proteinosis, interstitial lung disease, pulmonary adenocarcinoma, pulmonary haemorrhage, cryptogenic organising pneumonia and bacterial pneumonia.13 To provide care for patients with ‘crazy paving’ on chest CT, a thorough investigation into the different causes should be undertaken but COVID-19 should remain high on the differential due to its increasing prevalence.
Nasopharyngeal swabs remain the primary confirmatory test for COVID-19. As suggested by the US Centers for Disease Control and Prevention, negative results should not be the sole determinant to rule out COVID-19 infection. The optimum specimen type and peak viral levels have not been determined, and to detect the virus, multiple specimens at different time points may be required. False negatives may also occur if a specimen is improperly collected or processed or if an inadequate number of organisms are present. Ultimately, the positive and negative predictive values of the test are dependent on prevalence of the disease.14 There have been three published case reports of initially negative COVID-19 PCR tests in patients subsequently determined to have COVID-19 infection.15 16 Other sites of collection were recently tested in confirmed cases of COVID-19 with bronchoalveolar lavage specimens showing the highest positive results (93%) followed by sputum (72%), nasal swabs (63%), faeces (29%), blood (1%) and urine (0%).17 Even though bronchoalveolar lavage and sputum have higher positive results, these should be avoided due to the possibility of aerosolisation of the virus and potential exposures to healthcare workers in the setting limited healthcare resources.
This patient had several laboratory abnormalities that have been associated with worse outcomes including a serum neutrophil/lymphocyte ratio >3,18 D-dimer >1000 ng/mL19 and total lymphocyte count <0.8 (table 1).19 It is important to draw labs on presentation and periodically monitor throughout hospitalisation to project a patient’s trajectory.
When a patient is ultimately able to return home, quarantine is essential to preventing further spread of the virus. A test-based strategy is currently recommended to clear the patient from isolation which involves fulfilling all criteria including resolution of fever without antipyretics, improvement in respiratory symptoms and two negative COVID-19 PCRs at least 24 hours apart.20 This strategy may change based on the effectiveness of contact tracing and transmission of COVID-19 prior to onset of symptoms or isolation.21 At present, quarantine and negative COVID-19 PCR confirmation remains the cornerstone in preventing transmission.
Finally, this case presents important public health considerations including how to allocate scarce critical care resources in a public health emergency. Previously straightforward conversations with patients regarding their resuscitation status will change in a public health emergency. The act of performing cardiopulmonary resuscitation (CPR) on a patient with COVID-19 potentially increases viral transmission to healthcare providers and requires use of scare personal protective equipment that could be used on patients with a higher chance of recovery. It has been suggested that attending physicians, during this COVID-19 pandemic and a public health emergency, may withhold CPR from patients with or without COVID-19 if they deem CPR to not be medically appropriate, even at the dissent of the patient or their representative. ‘Medically appropriate’ is a term that takes into account the risk to healthcare workers performing CPR, the patient’s prognosis if CPR was successful and that the patient would remain a priority to continue receiving critical care resources following CPR.22 Creation of an independent triage team with allocation criteria for intensive care admission and ventilation based on likelihood of long-term survival may also become important. This type of framework provides the greatest amount of help to the greatest number of people.23 Ultimately, if we are faced with a public health emergency and triage of scare resources, we will need to employ effective crisis leadership skills. These skills include being adaptable, empathetic, prepared, resilient, transparent and trustworthy. Leadership during a crisis includes making decisions not based on reputation but rather based on the values of the group, organisation and community that the provider represents.24
Learning points
Nasopharyngeal severe acute respiratory syndrome-coronavirus-2 PCR does not have 100% sensitivity. It is affected by specimen collection and optimum peak viral levels. At this time, it is unknown when viral levels peak in patients with COVID-19 infection.
Clinical suspicion complemented by CT imaging is therefore paramount in the diagnosis. If clinical suspicion remains high after an initial negative nasopharyngeal swab, a swab can be repeated later in the time course.
Such vigilance can maximise positive outcomes for patients, reduce community transmission and strength ongoing efforts including physical distancing.
Footnotes
Contributors Supervised by SBD. Patient was under the care of MS, AK, AMP and SBD. Report was written by MS, AK, AMP and SBD.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.