Article Text

Statistics from Altmetric.com
Description
A 50-year-old man presented to the emergency department with fever, altered mental status, incoherent speech and involuntary movements. He had a high-grade fever with upper respiratory symptoms 9 days prior, and was diagnosed with influenza B infection by rapid antigen test, for which he was prescribed antipyretics without antiviral medication. Over the 4 days prior to admission, he became gradually unarousable, with random incoherent speech and unintentional muscle twitching, prompting his family to bring him for evaluation. The patient had untreated hypertension and his family history was unremarkable.
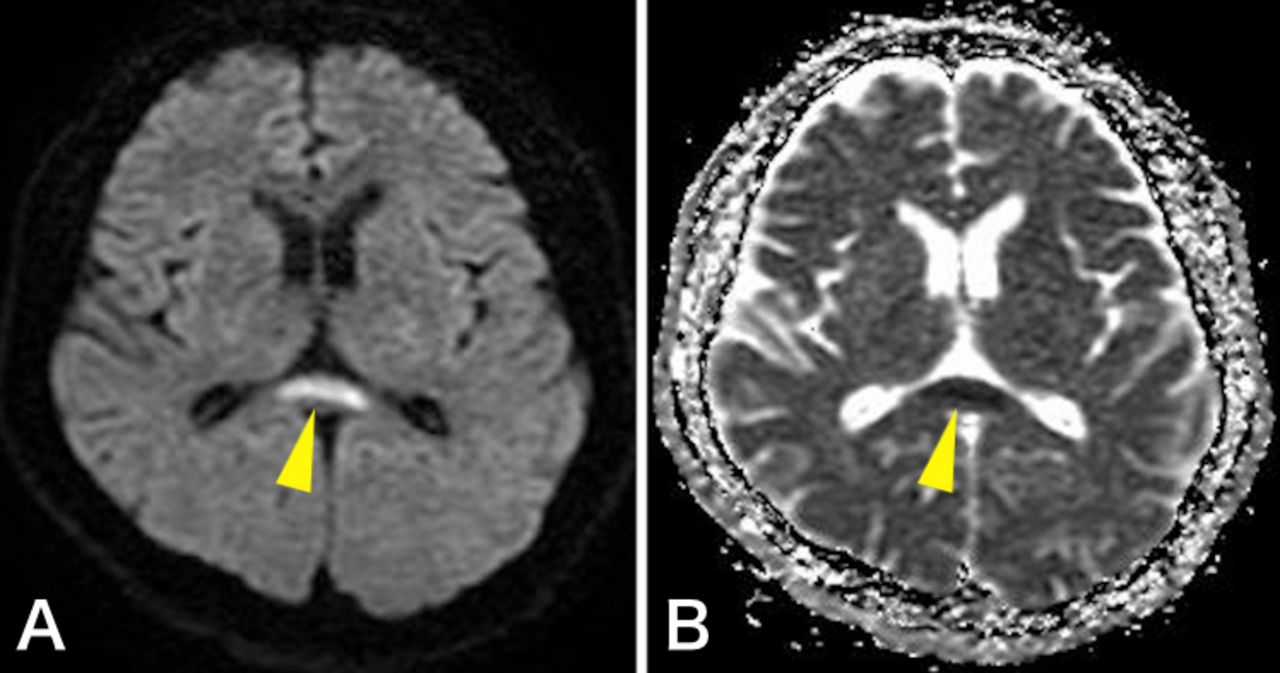
On presentation, his body temperature was 38.3°C and other vitals were unremarkable. He was disoriented to time and place. General examination was unremarkable, but neurological examination revealed myoclonus in both arms, an inability to stand on his feet and neck stiffness with a positive Kernig’s sign. Laboratory data showed mild hyponatremia (132 mEq/L). CT of the brain was unremarkable. Cerebrospinal fluid obtained from a lumbar puncture showed elevated white cells of 0.14×109/L with predominance of lymphocytes (98%) and a protein level of 257 mg/dL. An MRI scan of the brain revealed high intensity in the centre of the splenium of corpus callosum (SCC) on diffusion-weighted imaging (DWI) (figure 1A). Hypointensity in the same region was noted on an apparent diffusion coefficient (ADC) map (figure 1B) indicating mild encephalitis/encephalopathy with a reversible splenial lesion (MERS) after influenza infection. The differential diagnosis of these MRI findings included splenial ischaemia, acute disseminated encephalomyelitis, multiple sclerosis and lymphoma.1

MRI of the brain revealed high intensity in the centre of the splenium of corpus callosum on diffusion-weighted imaging (A) and hypointensity on apparent diffusion coefficient map (B) (yellow arrowheads).
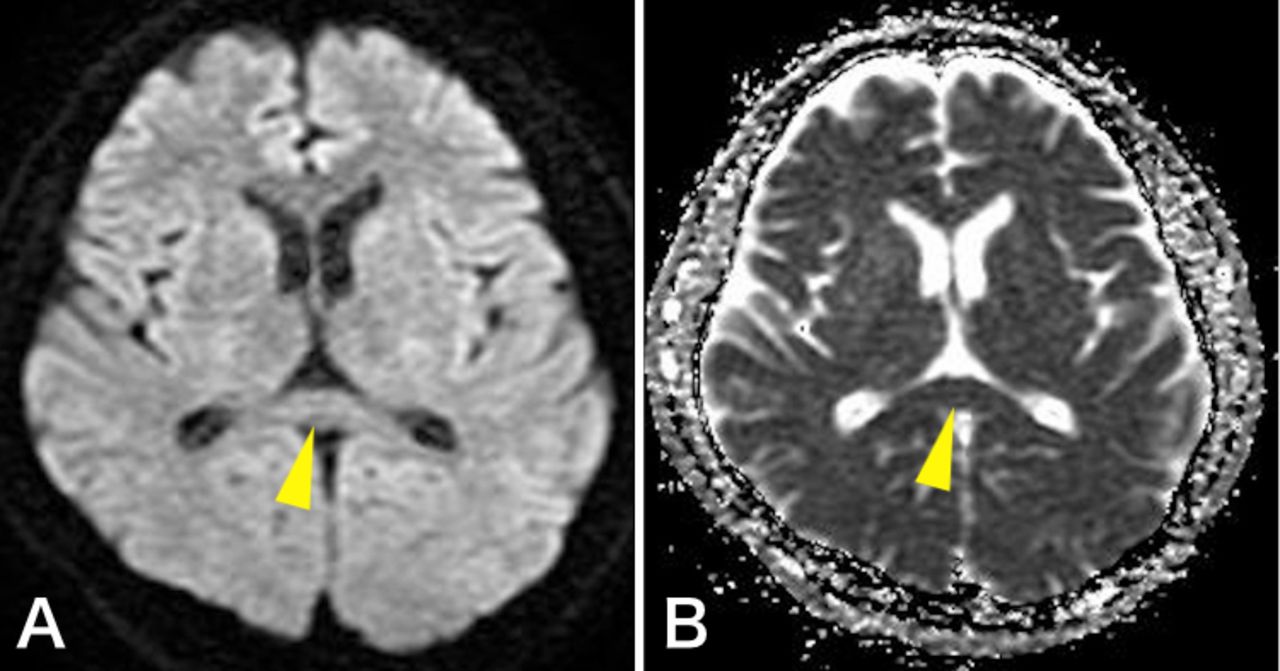
The patient was treated with intravenous acyclovir and cefotaxime until microbiology testing ruled out herpes simplex virus and bacterial meningitis. After 10 days of supportive care, there was nearly complete resolution of neurological symptoms. A follow-up MRI showed complete resolution of the high-intensity signal from the SCC (figure 2), establishing the diagnosis of MERS following influenza infection. The patient was discharged ambulatory on day 12.

{kind=link}
{kind=link}
Follow-up MRI of the brain showed complete resolution of the lesion on diffusion-weighted imaging (A) and apparent diffusion coefficient map (B) (yellow arrowheads).
MERS, not to be confused with Middle East respiratory syndrome due to coronavirus, was first described in 15 patients with acute but transient encephalitis/encephalopathy with characteristic splenial lesions.2 MERS is a clinico-radiological syndrome with a good prognosis characterised by transient MRI findings; high-intensity signals in the SCC were observed on DWI, T2-weighted images and fluid-attenuated inversion recovery images, along with low-intensity lesions on ADC maps.3 MERS is a well-known condition in children, but rarely occurs in adults. Clinical appearance includes central nervous system symptoms such as altered sensorium, seizures, delirium and headache. Complete recovery typically occurs within 1 month.2 MERS may follow viral infections such as influenza, mumps or rotavirus, and also bacterial infections such as Legionella pneumonia, Mycoplasma pneumonia or Salmonella enteritidis.3 The predilection of MERS for the SCC is unexplained, although hypotheses to explain the mechanism of MERS include intramyelinic axonal oedema, inflammatory infiltrates, oxidative stress and fluid imbalance.4
Early imaging, along with comprehensive evaluation for meningitis, viral encephalitis or other neurological diseases, is necessary for the diagnosis of MERS.
Learning points
Mild encephalitis/encephalopathy with a reversible splenial lesion (MERS) is a clinico-radiological syndrome with a good prognosis characterised by transient MRI findings.
Clinical appearance includes central nervous system symptoms such as altered sensorium, seizures, delirium and headache.
MERS may follow viral infections such as influenza, mumps or rotavirus, and also bacterial infections such as Legionella pneumonia, Mycoplasma pneumonia or Salmonella enteritidis.
Acknowledgments
Dr Rita McGill edited language.
Footnotes
Contributors IT wrote the manuscript, collected data and contributed to overall writing. HY wrote the manuscript, collected and edited data and contributed to the entire manuscript. MK contributed to writing the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.