Article Text

Statistics from Altmetric.com
Description
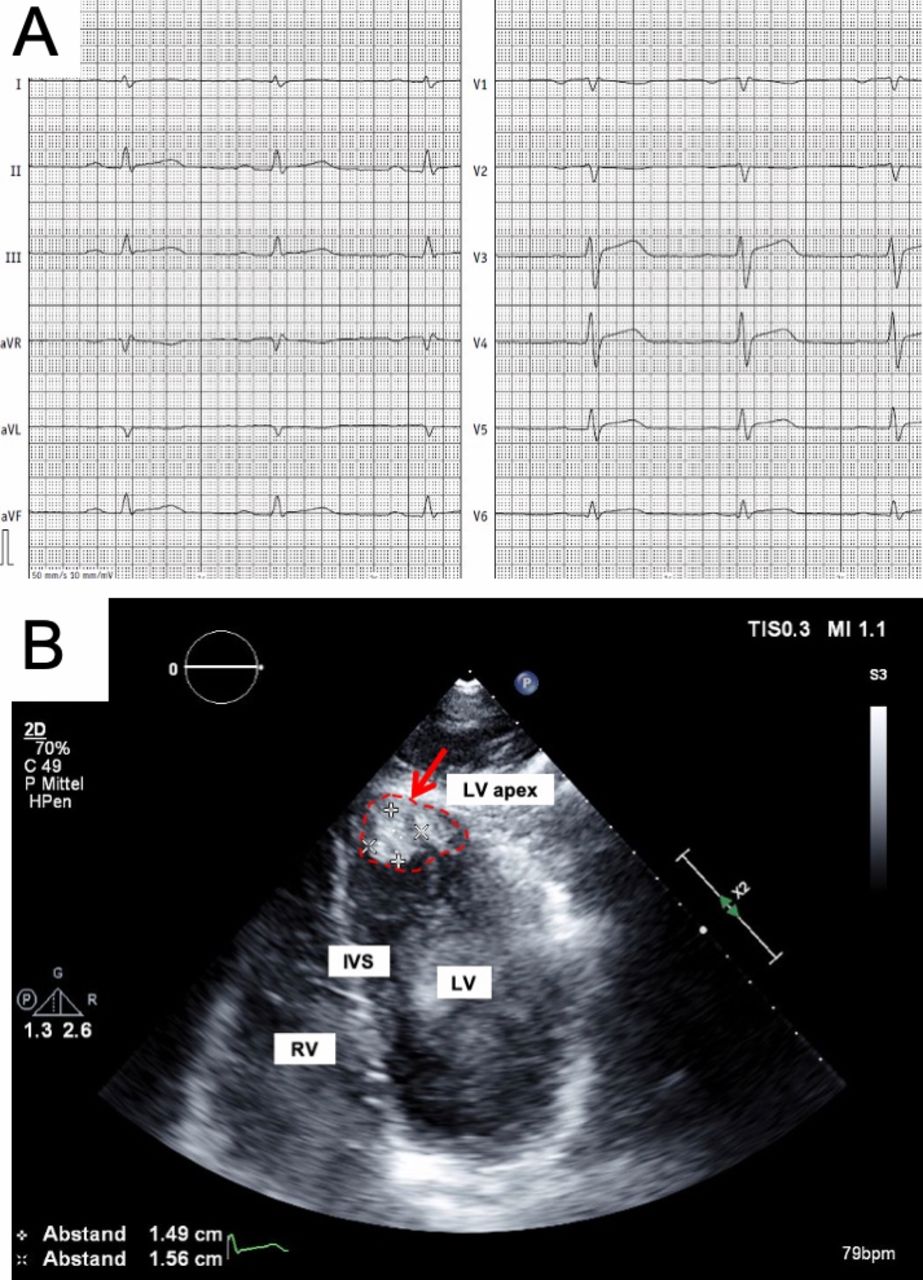
A 57-year-old male patient with a history of dyspnoea was admitted to the hospital for exertion, fatigue and joint pain experienced in the last month. The patient had been treated in another hospital for pneumonia with antibiotic therapy. The pneumonia did not improve, and the patient reported weight loss in the last months and experienced episodes of haemoptysis. Clinical examination revealed no abnormalities. The ECG showed elevated ST segments in the leads II, III and aVF as well as an inversion of the T waves in aVL, V1 and V2 (figure 1A). Troponin I was increased with 24 918.40 pg/mL (reference: <34.2 pg/mL). Further laboratory findings showed elevation of the C-reactive protein by 30 mg/L (reference: <2.0 mg/L) and an erythrocyte sedimentation rate of 81 mm/first hour (reference: <20 mm/first hour). Transthoracic echocardiography showed a reduced left ventricular ejection fraction of 40% and a left ventricular thrombus (figure 1B). Atherosclerotic obstructive coronary artery disease was excluded by coronary angiography. The examination presented most probably inflammatory obstruction of the distal Ramus interventricularis anterior with thrombus formation (figure 2A). MRI showed a delayed myocardial enhancement of the left ventricle myocardium (figure 2B). Further laboratory testing showed high positive autoantibodies against proteinase 3 (158.3 U/mL, reference: 1–10 U/mL) and cANCA (titre: 1:100, reference: negative). The final diagnosis based on the clinical and laboratory findings as well as imaging was granulomatosis with polyangiitis, with cardiac involvement.

(A) ECG with elevated ST segments (II, III and aVF) and inversion of the T waves (aVL, V1 and V2). (B) Transthoracic echocardiography with a reduced left ventricular ejection fraction (40%) and a left ventricular thrombus (red arrow and dotted line) (IVS, interventricular septum; LV, left ventricle; RV, right ventricle).

{kind=link}
{kind=link}
(A) Coronary angiography with absence of coronary heart disease (arrow: distal Ramus interventricularis anterior (RIVA) with thrombus formation; LCA: left coronary artery; RCA, right coronary artery). (B) MRI with delayed myocardial enhancement of the left ventricular myocardium (arrows).
Learning points
Granulomatosis with polyangiitis is a rare systemic inflammatory disorder characterised by vasculitis of the small arteries, the arterioles and the capillaries together with necrotising granulomatous lesions.
In rare cases, the disease shows cardiac involvement.1
Cardiac involvement is associated with increased troponin I and delayed myocardial enhancement as a sign of inflammation in small vessel vasculitis.
Footnotes
Contributors MF and AP treated the patient, reported the clinical course, designed the manuscript and interpreted the findings. DR performed important imaging studies of the patient, designed the manuscript and interpreted the findings. GW treated the patient and contributed to data interpretation.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.