Article Text

Abstract
Meningoencephaloceles of the skull base most commonly occur as a sequela of head trauma or they can more rarely be congenital malformations. Several types of encephalocele exist depending on anatomic features and localisation. Clinical presentation and symptoms can vary. Different methods of management and repair of the concurring skull base defects have been described and ranging vary from endoscopic to open surgical approaches. We report the case of a 56-year-old Caucasian woman with the diagnosis of right sided spontaneous transethmoidal meninoencephalocele. Clinical presentation of this rare pathology, methods of diagnostic and management and its outcome are presented. Spontaneous skull base meningoencephaloceles are rare entities, without clear underlying etiologies. Multidisciplinary management is recommended. The transnasal endoscopic approach provides a wide skull base exposure with more advantages and less morbidity in comparison with the conventional open approach.
- ear, nose and throat
- headache (including migraines)
- head and neck surgery
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
The incidence of congenital skull base meningoencephaloceles is estimated to be 1 in 35 000 births and they are usually asymptomatic.1 Multiple anatomical types of skull base meningoencephaloceles have been described and those vary depending on the localisation of the lesion from: transphenoidal, spheno-orbital, sphenoethmoidal, transethmoidal and sphenomaxillary.2
The pathway of encephaloceles in the skull base varies from one anatomical types to another: transsphenoidal encephaloceles passes through the body of the sphenoid. Spheno-orbital encephaloceles passes through the roof of the orbit or sphenomaxillary fissure. Sphenoethmoidal encephaloceles protrudes through the posterior ethmoid cells and the sphenoid. Transethmoidal encephaloceles passes through the cribriform plate into the nasal cavity. Sphenomaxillary encephaloceles protrudes through the sphenomaxillary fissure.2
Meningoencephaloceles are also classified anatomically into frontal, occipital, parietal and basal types.3 Transethmoidal encephaloceles are classified among the basal type and are located at the level of the anterior and middle skull base.
Acquired meninigoencephaloceles are most commonly a sequel of head and cranial trauma or iatrogenic causes.4 Benign intracranial hypertension-induced meningoencephaloceles remain a rare entity.
Clinical presentations varies accordingly to the anatomical localisation of the encephalocele, the skull base defect and the underlying etiologies. Nasal obstruction, spontaneous cerebrospinal fluid (CSF) rhinorrhea, intranasal polyps, recurrent meningitis and headaches are the most common symptoms of basal encephaloceles.5
We report the case of a spontaneous transethmoidal meningoencephalocele in a patient presenting with recurrent unilateral rhinorrhea and chronic headaches. Diagnosis and management by transnasal endoscopic surgical repair are presented. Outcomes and follow-up are documented.
Case presentation
A 56-year-old Caucasian woman presented with an intermittent unilateral rhinorrhea on the right side for several months associated with chronic ipsilateral fronto-temporal headaches. She was in good health and had no significant medical background or history of head trauma or any nasal or para-nasal sinuses surgery. She underwent a neurological evaluation and the diagnosis of chronic tension headaches with migraines component was made. A medical treatment was tried without any symptom improvement.
Due to the unfavourable evolution, she underwent a head CT scan (figure 1A,B) and MRI (figure 1C,D). These radiological examinations showed a cystic mass located in the anterior ethmoidal cells on the right side with an adjacent skull base bony defect. There were no other intracranial mass or other lesions. The rest of the nasal cavity and sinuses showed no other anomalies.
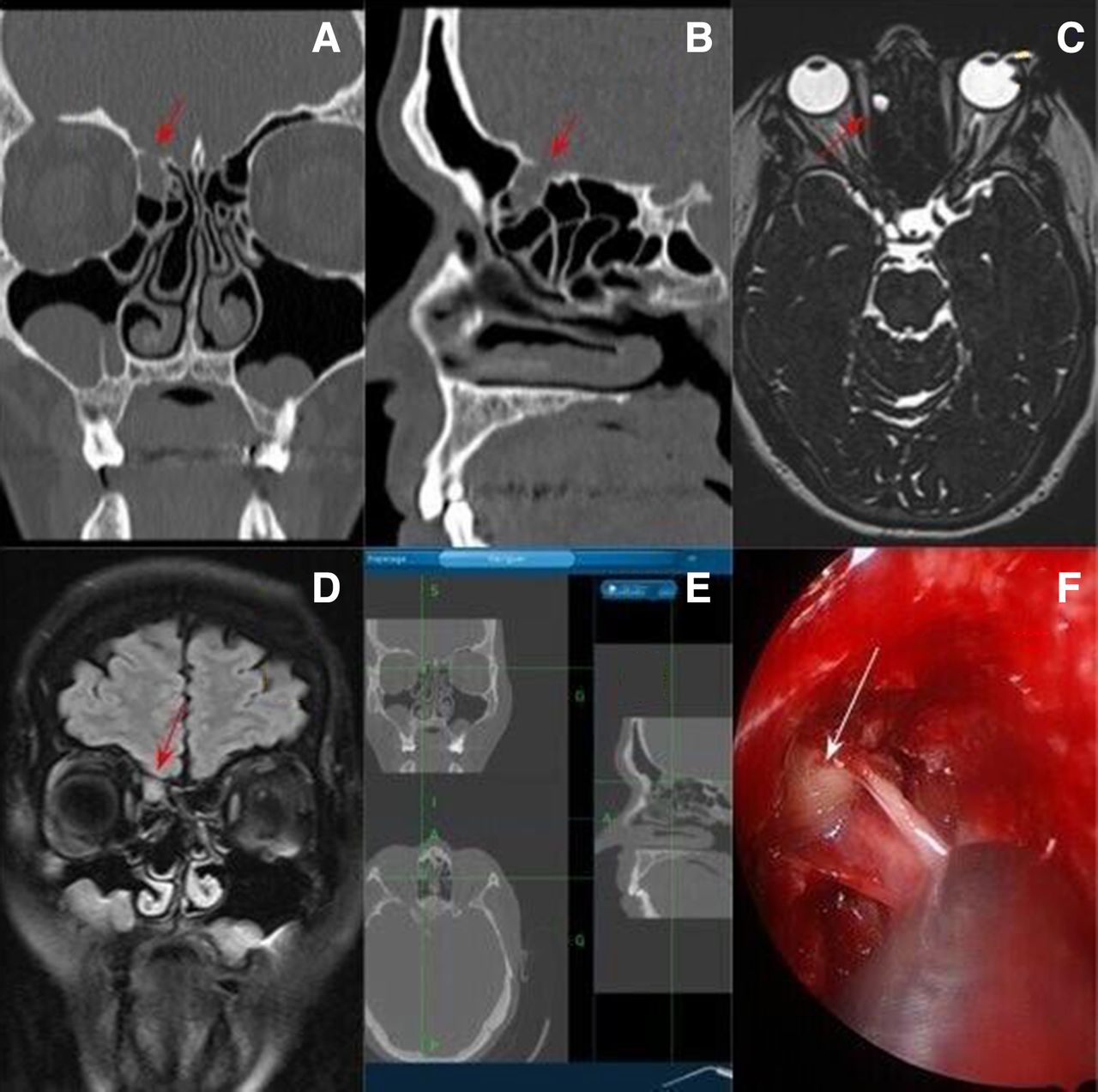
(A) Coronal CT scan view shows the lesion with a bony defect at the level of the skull base on the right side. (B) Sagittal CT scan view shows the lesion on the anterior ethmoid cells in the right side with a skull base defect at this level. (C) MRI imaging on T2 sequence fat sat, axial view shows the cystic lesion on the anterior right ethmoid. (D) MRI imaging on T2 sequence Fluid Attenuated Inversion Recovery (FLAIR), coronal view shows the cystic lesion on the anterior right ethmoid. (E) Intraoperative three-dimensional imaging guided navigation system view shows the accurate localisation of the lesion. (F) Intraoperative endoscopic view shows the herniated sac of brain parenchyma at the level of the anterior ethmoid in the right side.
The patient was referred to the ear, nose and throat department for evaluation. Her initial complaint was an intermittent right-sided rhinorrhea without nasal obstruction or any other symptoms. The fiberoptic endoscopic examination of the nose showed a normal appearance of the nasal mucosa, mild and non-obstructive septal deviation, no evidence of intranasal mass or polyps. There was no spontaneous right-sided rhinorrhea but the Dandy manoeuvre (head bent forward and downwards for a few minutes) triggered a right-sided clear rhinorrhea and the analysis of this nasal liquid was positive for beta-2 transferrin protein.
According to these clinical and radiological findings, the diagnosis of a transethmoidal meningoencephalocele was retained. After discussion with the patient, the decision of a combined otorhinolaryngology and neurosurgery management was made.
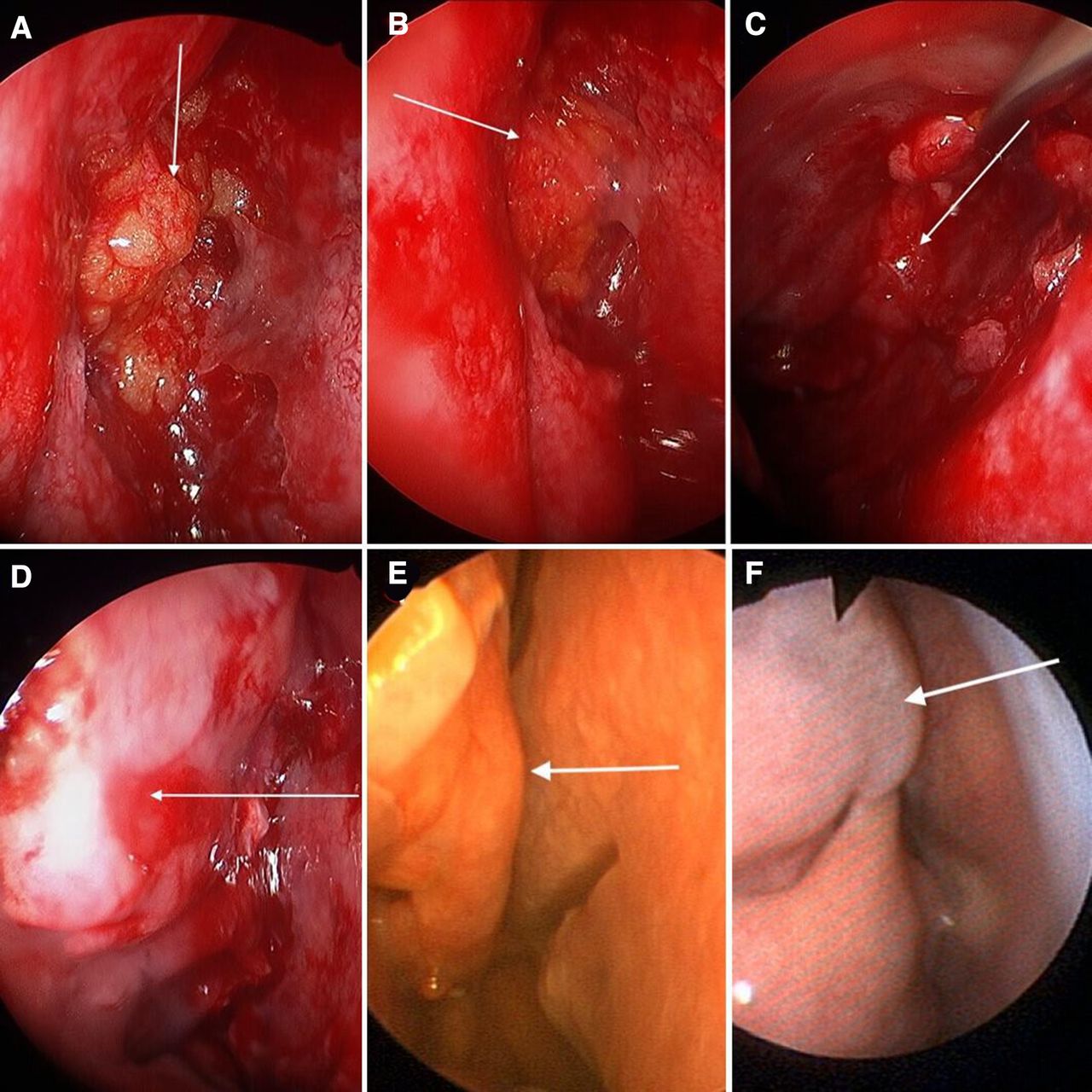
The surgical exploration and management was performed under general anaesthesia by a transnasal endoscopic approach using a three-dimensional image-guided navigation system (fusion ENT Navigation, Medtronic- Switzerland) with different types of nasal optics 0°, 30° and 45° (Karl Storz Endoscopy-Germany). A fat graft was harvested from the periumbilical area and a temporalis fascia graft was harvested from the postero-superior auricular region on the right side. The nasal cavity was prepared by topical application of vasoconstriction solution with local anaesthesia. An incision was made at the level of the head and the inferior border of the middle turbinate on the right side, the mucosa of the lateral surface of the middle turbinate was shaved using a microdebrider and the turbinate’s bone was partially resected with a total conservation of the upper insertion. An anterior right-sided ethmoidectomy was performed and the localisation of the meningoencephalocele in the anterior ethmoide cells was identified using the navigation-guided system (figure 1C,F). The neurosurgery team carried out the excision of the transethmoidal meninigoencephalocele using a bipolar electrical cauterisation and cold instruments to achieve a complete resection of the cerebral tissue forming the lesion. The bony defect on the anterior ethmoidal skull base was closed in three layers. The fat grafts was applied on the deep plane, then followed by the temporalis fascia graft on the middle plane and both grafts were fixed with tissue glue. A flap of the residual mucosa of the right-sided middle turbinate was rotated laterally and up into the skull base defect and used as the third and superficial layer of reconstruction, which was fixed by using a tissue glue (figure 2A–D). The right nasal cavity was then filled with rebsorbable packing.

{kind=link}
{kind=link}
(A) Intraoperative endoscopic view shows the first layer of reconstruction of the skull base defect with a fat grafts. (B) Intraoperative endoscopic view shows the application of the fat grafts at the level of the defect and fixation with a tissues glue. (C) Intraoperative endoscopic view shows the second layer of reconstruction of the defect by using, a fascia lata graft fixed with tissues glue. (D) Intraoperative endoscopic view shows the third layer of reconstruction using a mucosal flap of the middle turbinate fixed with tissues glue. (E) Three months postoperative endonasal endoscopic view shows a complete closure of the skull base defect. (F) One-year postoperative endoscopic view shows a longtime stability of the reconstruction with a good aspect of the middle turbinate flap.
The patient was kept under observation in the intensive care unit for 5 days with strict bed rest and head at a 45° flexion head position. A prophylactic antibiotic was introduced (amoxicillin 1 g, two times per day for 7 days) with closed monitoring of inflammatory and biological parameters. No postoperative complications were observed. The patient was discharged 1 week after the surgery. The histologic analysis of the resected spaceman showed a brain tissue without signs of malignancy.
Close ambulatory follow-up showed favourable recovery. No recurrence of the right-sided clear rhinorrhea or any neurological complications were observed. The frontal headaches were reduced with the persistence of intermittent pain, most likely related to the migraines already known to her. She was referred to the department of neurology for its management. Various lumbar punctures carried out preoperatively and postoperatively did not demonstrate any signs of intra cranial hypertension. All the different measurements of CSF opening pressure were within the normal limits (less than 200 mmH2O)
The follow-up at 1 year after the surgery showed absence of any right-sided clear rhinorrhea with a very acceptable result of the skull-base defect reconstruction (figure 2C,F).
Outcome and follow-up
There were neither intraoperative, nor postoperative complications.
Follow-up at 1 year after surgery showed no recurrence of unilateral rhinorrhea nor any other symptoms apart from the milder, intermittent know migraines.
Endoscopic control at 1 year showed a good and stable aspect of the skull base reconstruction.
Discussion
Skull base encephaloceles in adult patients remain uncommon entities and most frequently occur in a context of head trauma or iatrogenic injury.6 Spontaneous encephaloceles at the level of the skull base are very rare conditions and estimated to occur in only 3%–5% of all cases of CSF leaks.7 The role of idiopathic intracranial hypertension as a predisposing factor for development of spontaneous skull base encephaloceles has been suggested in a previously reported case series.8 The association between spontaneous encephaloceles and dural arteriovenous fistula with intracranial hypertension in pregnancy patients has been reported in the literature.9–11
Many other hypotheses regarding the physio pathogenesis of the skull base encephaloceles have been proposed; McLaurin et al have suggested the role of a defect of closure of the anterior neuropore at the fourth week of pregnancy,12 an increase in intraventricular pressure could occur during development and would be responsible for passage of cerebral parenchyma through a bony zones of least resistance. The variation of the CSF pressure was discussed by Rovit et al.13 Some small encephaloceles could be formed in a zone of bone weakness or congenital bone defect in response to pulsatile CSF. The formation of a bone and dural defect could be related to a multiple anatomical factors; the thin nature of the skull base bones, later development of the skull base and the lined by adherent dura mater on the upper surface with fragile mucosa on the lower surface.1
The management of this rare and little-known pathology must be based on a multidisciplinary cooperation and regarding the literature, the best outcomes and results are obtained by a multidisciplinary team of neurosurgeons and otolaryngologists.14 The main objective of surgical management is to resect the non-functional brain parenchyma herniated inside the sac and reconstruct the defect of the skull base in order to isolate the cranial fossa from the sinonasal cavity. Many different surgical approaches have been described in the literature and those varies from conventional open surgery to endonasal endoscopic approach. The endoscopic offers more advantages by providing better quality close-up view, panoramic vision of anatomic landmarks and satisfactory exposure of the skull base.
The reconstruction of skull base defects could be done by using different techniques and type of filling material depending on the size, localisation of defect, underlying pathology and surgical experience. Two layers reconstruction methods using different materials, such as fascia lata, fat graft and septonasal flap were used by the majority of authors.
In our case presented above, the diagnosis of spontaneous transethmoidal meningoencephalocele seems the most likely in absence of a clear underlying pathology. Most importantly, the different CSF pressure measurements performed did not confirmed the hypothesis of benign intracranial hypertension. However, we believed that our patient could have predisposing factors, such as a possible weakness of the bony skull base at this area associated with variations of the intracranial pressure.
Our decision to reconstruct the defect of the skull base in three layers was made in order to achieve a strong and longstanding repair. Lauren et al15 suggested that middle turbinate (MT) preservation is not appropriate for skull base defects located lateral to the MT attachment and in these cases, MT resection is necessary for a better exposure of the defect. In our case, we used a mucosal flap of the MT as a third layer of reconstruction without MT resection and we had no difficulties neither in the exposure, nor in the mobilisation of the flap laterally into the defect.
Learning points
Spontaneous transethmoidal meningoencephaloceles are rare entities with no underlying clear etiologies.
The role of predisposing skull base anatomic conditions and the variations of spontaneous cerebrospinal fluid pressure is to be considered in this pathology.
Multidisciplinary team management is widely recommended, with high successful rate and better outcomes.
Transnasal endoscopic approach with three-dimensional imaging-guided navigation system carries more advantages and less morbidity.
Multilayer reconstruction of the skull base defect provides solid, longtime support with deceasing of recurrence.
Footnotes
Contributors BH: Reporting, corresponding author and design. ARK: Acquisition of data. JYF: Reporting, acquisition of data. SB: Reporting.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.