Article Text

Statistics from Altmetric.com
Description
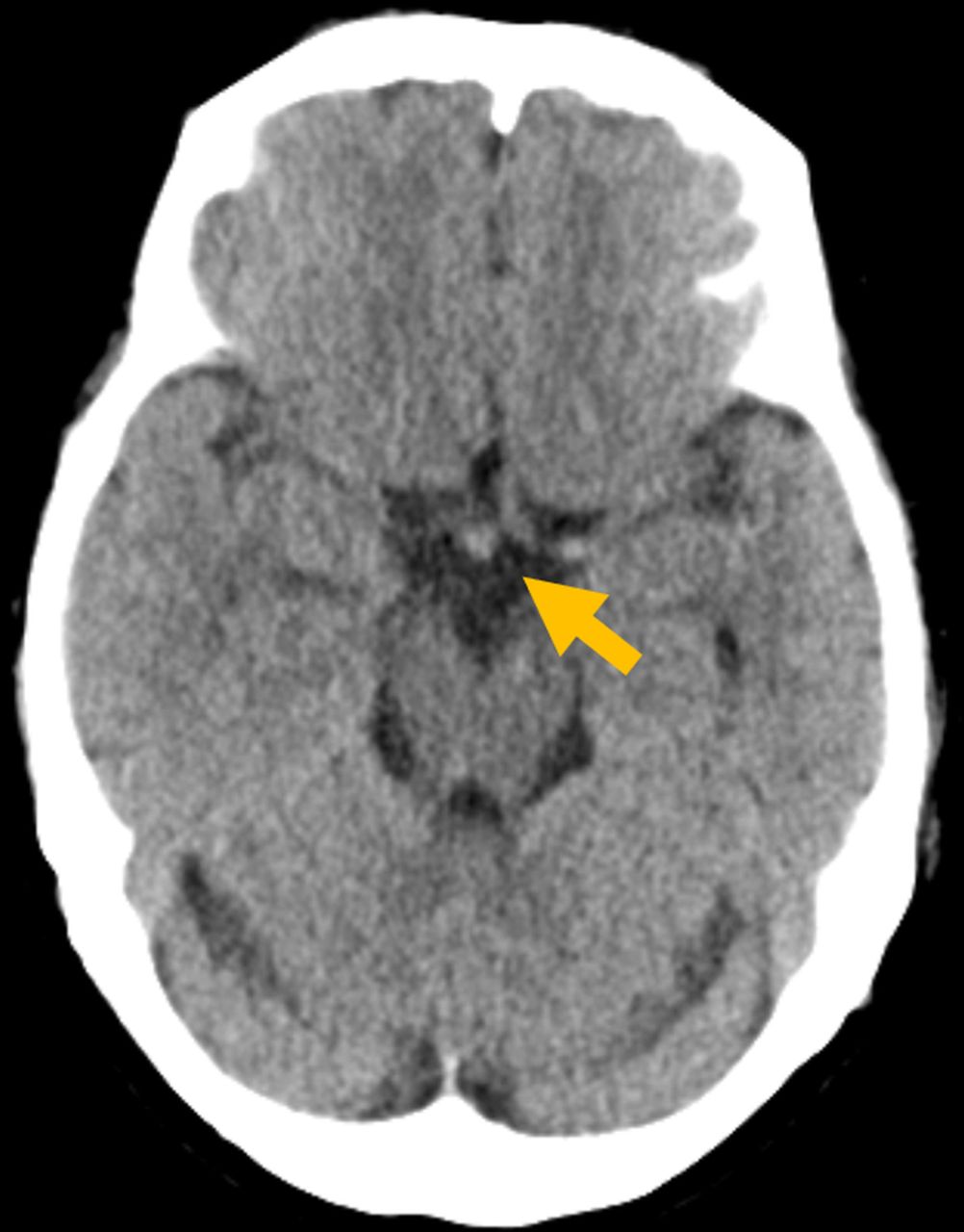
A 54-year-old woman presented with transient headache underwent CT scan, which revealed a high-density 6 mm lesion of the diencephalon (figure 1). Her headache subsided overnight. She was born 1300 g at 7 months of gestation, but grown healthy except for euthyroid Hashimoto disease and dyslipidaemia. MRI revealed normal-sized anterior pituitary within the sella turcica (figure 2A). However, the stalk was unidentifiable and T1-high-signal corresponding to the neurohypophysis was missing in situ (figure 2A), but present beneath the median eminence (figure 2A,B). High density lesion visualised by CT scan was also identifiable by the axial view of the MRI study (figure 2C). On MRI, the lesion was just posterior to, but not attached to the optic chiasm (figure 2C). Serum and spot urine osmolality, and antidiuretic hormone levels were 288 mOsm/kg, 784 mOsm/kg, and 0.6 pg/mL, respectively, arguing against the presence of diabetes insipidus. Anterior pituitary hormones were normal, except insulin-like growth factor-I (IGF-I) (43 ng/mL, mean±2SD: 76–211) without symptoms or signs of growth hormone (GH) deficiency. Serum IgG4 was normal and antipituitary antibodies negative. Blunted stalk with typical T1-high-signal of the posterior pituitary lobe outside the sella supports the diagnosis of ectopic posterior pituitary.1 It is a rare condition with or without hypopituitarism.2 Perinatal trauma or mutations of the transcription factors regulating pituitary development (HESX1, LHX4, OTX2, SOX3) are reported as aetiology.2 The results of the imaging study in this patient remained unchanged 13 months later.

Brain CT scan image without contrast enhancement revealed a nodular region of similar density to brain parenchyma (arrow) anterior to interpeduncular cistern and posterior to optic chiasm.

{kind=link}
{kind=link}
MRI scan images. (A) Sagittal view T1-weighted image. Soft tissue intensity of normal size was present within the sella turcica (arrowhead), but high intensity signal corresponding to the posterior lobe of the pituitary was absent orthotopically. Pituitary stalk not observed, and T1-high signal was found up at the tip of the infundibulum (arrow). (B) Coronal view T1-weighted image. T1-high signal just beneath the optic stalk (arrow). (C) Axial view fluid attenuation inversion recovery (FLAIR) image. High intensity lesion (arrow) was identified just posterior to the optic chiasm.
Patient’s perspective
I was surprised to hear that my brain is a bit different from the others because I have always thought that I am healthy. But I feel relieved now to hear that the unusual position of a part of my brain is not and may not be causing serious harm to my everyday living.
Learning points
Ectopic posterior pituitary may be discovered in brain imaging incidentally in adults.
Ectopic posterior pituitary may appear as a diencephalic mass in CT scans.
Screening for anterior as well as posterior pituitary hormones are recommended in incidentally-identified ectopic posterior pituitary.
Acknowledgments
The authors are grateful to Professor Hiromi Kataoka for supervision and to Ms Aya Nakamura for clerical assistance.
Footnotes
Contributors TT and HO have been in charge of the patient care. HK and DA gave advises in clinical management and manuscript preparation as consultant endocrinologists.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.