Article Text

Abstract
Cervicofacial actinomycosis remains a rare pathogenic finding in the paediatric population. Diagnosis is challenging, as findings are often non-specific and Actinomyces species are generally difficult to culture. Treatment is a prolonged course of antibiotics, either intravenous and oral, often combined with a surgical procedure to remove the lesion. This patient had non-specific intermittent left mandibular pain for 8 months that was eventually attributed to an Actinomyces odontolyticus infection in the mandible. Diagnosis required incisional biopsy, and treatment involved 12 months of oral antibiotics.
- dentistry and oral medicine
- infections
- bone and joint infections
- mouth
- oral and maxillofacial surgery
Statistics from Altmetric.com
Background
Actinomyces species are slow-growing facultative anaerobic bacteria, and cause a chronic disease manifesting with fistulas, abscess and chronically inflamed tissues. Cervicofacial variants, actinomycosis’ most common manifestation, account for about half of the cases and can also be frequently seen in the pulmonary system and central nervous system.1 Infections tend to result from a localised insult to the mucosal tissue, whether from trauma or dental infection.2 3 Actinomyces species, like fungi, maintain a filamentous appearance, but do not grow spores and thus are classified as bacterial.4
Actinomycosis infections almost always manifests as part of a polymicrobial infection, often with oral anaerobes such as streptococcus, gram-negative rods and other fusiform bacteria. These other bacteria can either provide the cofactor toxin, tissue-decomposing enzymes such as hyaluronidases, or inhibit the host immune response to allow for actinomyces invasion.5 6 Actinomyces bacteria are notoriously difficult to culture due to their slow-growing nature and the fastidious conditions with temperature and carbon dioxide content that are necessary, and can take up to 21 days for adequate growth.7 It is also a relatively rare infection, with nearly 80% of cases in the adult population, and for unknown reasons, manifests with a male predisposition with a near 2:1 ratio in adults.8 9 Actinomycosis infections are usually treated with long-term antibiotics, with PO showing as similar clinical efficacy as intravenous antibiotics for milder cases. Combined surgical debridement is also indicated in some circumstances.10
This is a report of a paediatric actinomycosis infection of the mandible that manifested as pain and swelling for a prolonged period of time. The patient was treated with surgical debridement and long-term antibiotic treatment. The goal of this report is to highlight the importance of a surgical biopsy, culture and histopathological evaluation of any mandibular or maxillary process that results in swelling and pain. A review of the current literature on clinical manifestations, diagnostic techniques and treatment methodologies was also performed.
Case presentation
A 10-year-old girl with no significant medical history was referred to the Oral and Maxillofacial Surgery clinic after about 8 months of waxing and waning left sided mandible pain and swelling. Throughout her initial presentation she denied erythema or drainage. Her family reported no history of facial trauma, dental procedures or dental caries. Early on in her presentation, her symptoms were initially attributed to an odontogenic infection. However, her paediatric dentist was unable to find any offending odontogenic source or periodontal disease.
Investigations
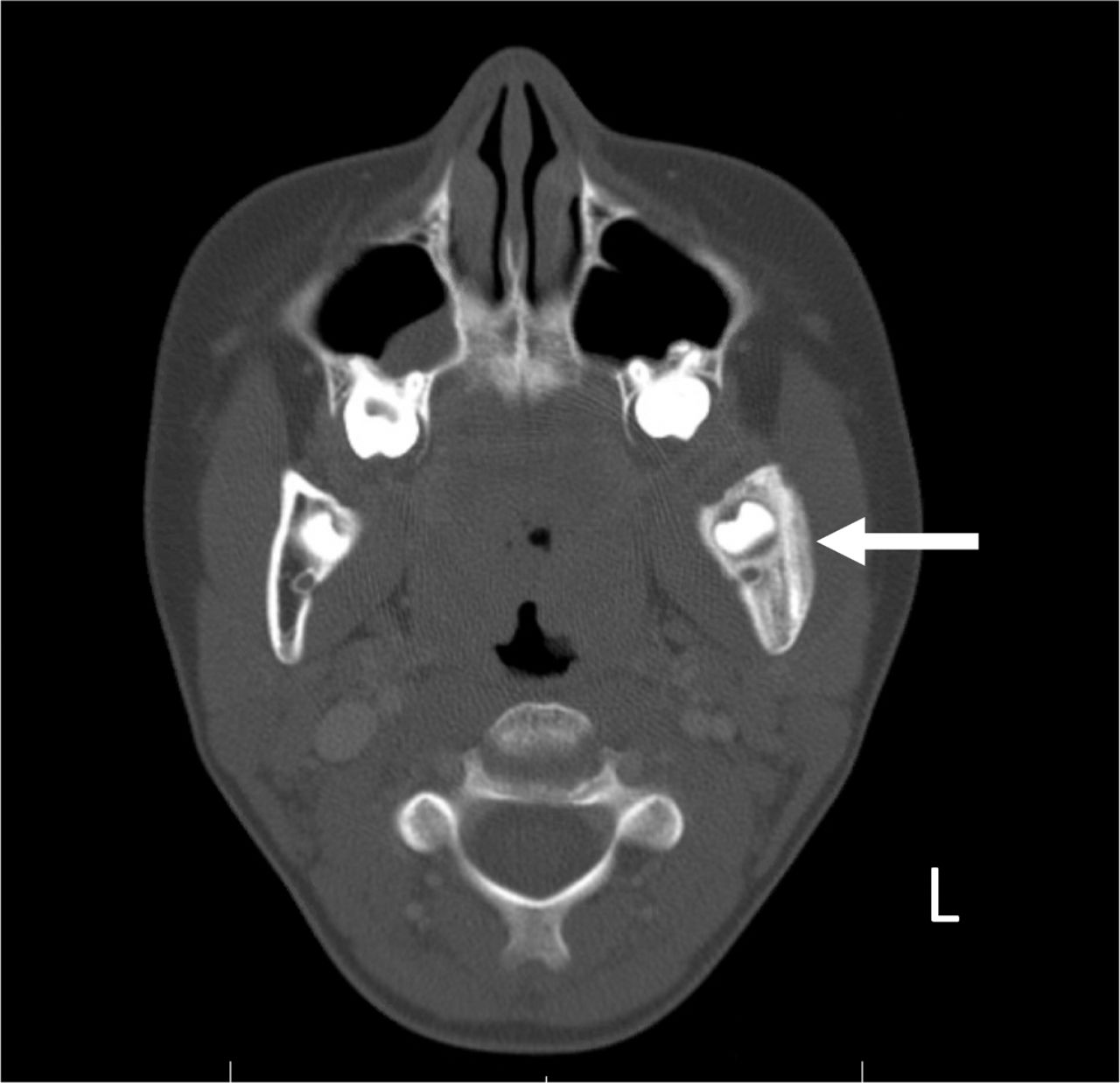
The patient was eventually evaluated by her paediatrician, who referred her to an otolaryngologist, who subsequently referred her to our clinic. She did report intermittent fevers, most notably once to Tmax of 40°C. During those episodes, she presented to the local children’s hospital emergency department (ED) for evaluation and short courses of intravenous antibiotics. Complete blood count labs at those times were within normal limits. The ED staff placed her on several courses of penicillin-class oral antibiotics. She unfortunately was notably non-compliant due to her dislike of the medication taste. Oral steroid courses were also prescribed with no improvement in facial swelling. A posterior–anterior cephalometric radiograph was taken that revealed early reactive changes in the left mandible ramus, but was not noted on formal read (figure 1). Prior to her presentation in our clinic, a contrast-enhanced neck CT was performed in the ED which revealed bony expansion of the left mandible and overlying soft tissue swelling on both axial and coronal views (figures 2 and 3).

Posterior–anterior cephalometric radiograph. Early reactive changes can be seen in left mandibular ramus prior to her presentation in our clinic.

Maxillofacial CT with intravenous contrast, axial view, black arrows highlighting periosteal thickening and layering in left mandible ramus with surrounding soft tissue oedema.

Coronal view again demonstrating thickening of the periosteal layer in left mandible ramus. Arrow points to periosteal reaction.
After her initial presentation, we obtained a contrast-enhanced MRI to better characterise her mandibular lesion. The MRI resulted in a hyperintense T2 signal abnormality in the left mandibular bone marrow with periosteal thickening suggestive of a chronic infection or chronic recurrent multifocal osteomyelitis (figure 4). No drainable fluid collection was seen. During her preoperative evaluation, her intraoral findings revealed clinically healthy periodontium with only mild tenderness on palpation (figure 5).

T2-weighted MRI, axial view demonstrating reactive periosteal changes (white arrow) with hyperintense signals in the adjacent soft tissues (yellow arrow).

Preoperative intraoral view demonstrating pink, well-perfused and healthy tissue in left posterior mandible area without evidence of periodontal or dental disease.
Differential diagnosis
The clinical differential diagnosis typically includes odontogenic infection, periodontal disease, acute versus chronic osteomyelitis or a permeative paediatric tumour such a primary osseous lymphoma, Ewing’s sarcoma. However, she had benign clinical examination and radiographs of her dentition and periodontium. She also did not exhibit many of classic ‘B symptoms’ of cancer, having only intermittent fevers and non-specific mandible pain. Gram staining of Actinomyces bacteria reveal beading gram-positive bacilli with branches, which could be confused with Nocardia, as Nocardia bacteria often present with similar histological and clinical symptoms. However, Nocardia infections manifests primarily in immune-compromised patients as an opportunistic infection in the lungs, bones and joints. To differentiate, Nocardia bacteria have mycolic-acid content in their cell walls and thus are partially positive on acid-fast stains, and can also be grown in standard blood culture media, unlike the non-acid-fast staining anaerobic Actinomyces bacteria.
Treatment
The patient was brought to the operating room for an incisional biopsy culture under a brief general anaesthetic. Bovie electrocautery was used to create an intraoral incision along the left anterior ramus. A subperiosteal dissection was carried out exposing the ascending ramus. A corticotomy was carried out using a 1.2 mm fissure bur with a handpiece. There were no granules encountered during the procedure. Bony tissue was then submitted along with marrow for anaerobic, aerobic and fungal cultures. A piece of thickened periosteum was also submitted for frozen section, which was only revealed normal fibro-adipose tissue, skeletal muscle with mild oedema and minimal interstitial fibrosis. Bone was also sent for frozen section demonstrating expanded medullary spaces with oedema and vascular proliferation with no cytological atypia, staining positive for CD31, which demonstrated the presence of endothelial cells, but was negative for D2-40 and PROX1.
The final pathology resulted in generalised non-specific bony vascular proliferation that was negative for malignancy. Anaerobic cultures returned as Actinomyces odontolyticus. Tissue culture was negative for fungal and acid-fast bacilli. The surgical infectious disease team was consulted, who confirmed the diagnosis of cervicofacial actinomycosis and recommended the patient be placed on long-term antibiotics. An initial 6-month course of oral amoxicillin 1000 mg two times per day was prescribed. The patient tolerated the procedure well and was placed on routine monthly follow-up.
Outcome and follow-up
The patient responded well at her first monthly post-op visit with occasional mild pain in her mandible. At her fifth month visit, she reported continual, but less frequent, left mandibular pain and was sent for a repeat maxillofacial CT, which revealed signs of resolving/chronic osteomyelitis. She was subsequently seen by surgical infectious disease physicians who extended her antibiotic treatment to a 12-month course. She continued to improve and currently is doing well on oral antibiotics (figures 6 and 7).
Maxillofacial CT with intravenous contrast, axial view, 5 months after diagnosis. The study reveals resolving periosteal inflammation (white arrow) and resolving/chronic osteomyelitis.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Coronal view maxillofacial CT 5 months after diagnosis demonstrating resolving periosteal inflammation (white arrow).
Discussion
The Actinomyces family of infections have several different subspecies. The most common include Actinomyces israelii, Actinomyces naeslundii, Actinomyces bovis and A. odontolyticus. Sulfur granules and collections of Actinomyces filaments, are pathognomonic. However, these findings are not always seen, as in the case of this patient. The angle of the mandible is the most common cervicofacial location, manifesting as a firm extraoral swelling. It is thought that the mandible, with relatively poor vascularity compared with the rest of the midface skeleton, may predispose itself to infection.11 Fortunately, cervicofacial actinomycosis infections tend to respect tissue planes.12
This case report is unique in that the patient had no clear aetiology of a localised insult and is not immunocompromised. She reported no incidence of facial trauma, dentoalveolar procedures, periodontal disease or carious dentition that may have served as an entry point. In previous case reports, a localised infection or traumatic event generally served as the vehicle for Actinomyces bacteria to enter deeper tissue layers facilitating an anaerobic environment and further growth. This typically is required to produce an infection as Actinomyces bacteria themselves do not have the factors or enzymes to decompose tissue.13 14
Diagnosis of actinomycosis is notoriously difficult to diagnosis due to the fact that Actinomyces bacteria are quite difficult to culture. Histopathological evaluation is also routinely recommended, as these species stain positive for H&E, PAS (Periodic acid–Schiff stain) and Giemsa.15 PCR and nucleic acid probe techniques are available as well for actinomyces identification, though they are more time-consuming and expensive.6
Once a diagnosis of actinomycosis is made, antibiotic monotherapy is normally started, which has been reported as curative. Penicillin drugs are commonly first-line, with clindamycin or macrolides as alternative in penicillin-allergic patients. The duration of treatment should be guided by the severity of the disease, and the regiment is often institution-dependent, with total duration ranging anywhere from 2 weeks to 12 months. The logic behind the extended course is that Actinomyces bacteria tends to lyse at slower rates.16 In severe cases, such as those with presence of fistulous tracts or recurrent abscesses, patients can start with intravenous antibiotics and be transitioned to PO antibiotics once clinically improving.10 17 Antibiotic duration may also depend on whether concurrent surgical debridement was undertaken to healthy tissue borders.
In a case series of actinomycosis involving the mandible in paediatric patients, Robinson et al recommended starting with 3 months of oral antibiotic postdebridement, and then serial debridement if warranted on repeat imaging.12 Surgical therapy alone is rarely considered successful as definitive treatment.10 Barnard et al in 2013 wrote in a retrospective review that only a month of antibiotics was required to clear infection in 19 patients with cervicofacial actinomycosis, in conjunction with surgical therapy.16 Overall, prognosis of complete resolution is generally good, with low rates of recurrence after adequate treatment.18
To the best of our knowledge, search of the current literature for paediatric cervicofacial actinomycosis patients reveals a total of 28 cases. Of those, 15 were isolated to the mandible. This pathogen remains a relatively rare infection in the paediatric population. Interestingly, in paediatric case reports, female patients predominate for unclear reasons.19 Although actinomycosis infections are rare, any persistent facial swelling and pain should be evaluated for cervicofacial actinomycosis, especially if associated with recent dento-alveolar trauma or surgery such as dental extractions or root canal therapy. Delayed diagnoses are common as infection may not cause pain until later stages of the infection.20 Early intervention should prevent future complications such pathological fracture or extraoral manifestations such as a suppurative fistula.
This is a report of a paediatric actinomycosis case in a previously healthy 10-year-old girl who presented with left mandibular pain and mild swelling for a period of 8 months. She denied a history of trauma, recent dental procedures, periodontal disease or dental caries. Initially, she was thought to have dental caries; however, was cleared by her paediatric dentist. After an 8-month presentation, her final operating room (OR) culture grew A. odontolyticus, providing a diagnosis of cervicofacial actinomycosis. She was placed on an extended course of oral amoxicillin for 6 months, which was extended for a total of 12 months in order to treat this stubborn organism.
Learning points
This patient had non-specific symptoms that eluded diagnosis for nearly a year and did not get adequate treatment as a result. Early three-dimensional imaging is indicated when clinical examination or plain radiographic films do not provide the necessary information for a diagnosis, and if warranted based on the imaging, timely referral to a surgeon for a biopsy is vital.
While more common in the adult population, actinomycosis infections should be considered when evaluating paediatric intraosseous lesions as well.
Overall, this case report shows that actinomycosis infections, though rare in paediatric population, should be a diagnosis every clinician should keep on their list of differential diagnoses when evaluating mandibular pain and swelling.
References
Footnotes
Contributors RPS and JJC both equally contributed to the planning, conduct, reporting, conception and design, acquisition of data and interpretation of this case report.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Parental/guardian consent obtained.
Provenance and peer review Not commissioned; externally peer reviewed.