Article Text

Abstract
Critically ill patients are at risk of developing both acute kidney injury (AKI) and invasive fungal infections (IFIs). Prompt and efficient treatment of the IFI is essential for the survival of the patient. This article examines three distinct clinical situations where liposomal amphotericin B, a broad-spectrum antifungal agent, was successfully used in the setting of AKI. The first was Aspergillus infection in a 63-year-old man with bleeding oesophageal varices related to advanced liver disease. The second was gastrointestinal mucormycosis in a 74-year-old man who developed a small bowel obstruction following an autologous stem cell transplant for mantle cell lymphoma. The third was a Fusarium infection in a 32-year-old woman on immunosuppression for a bilateral lung transplant for cystic fibrosis. In all three cases, liposomal amphotericin B was required for urgent management of the patient’s IFI. We discuss the rationale for treatment with a potentially nephrotoxic agent in this setting.
- renal system
- safety
- acute renal failure
- infections
- drugs: infectious diseases
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Critically ill patients are at risk of developing both acute kidney injury (AKI) and invasive fungal infections (IFIs).1 2 AKI is a syndrome with multiple aetiologies characterised by an abrupt decrease in kidney function and an associated major increase in mortality risk.1 Prompt treatment of the IFI is critical for patient survival,3 but full diagnostic information is not always available to guide treatment choice. Empiric initiation of a broad-spectrum antifungal agent may therefore be necessary.
Amphotericin B has a broad spectrum of activity against organisms causing IFIs, but is associated with nephrotoxicity.4 The liposomal formulation is less nephrotoxic than conventional amphotericin B, but optimisation or maintenance of the patient’s renal function is an important consideration during its use.5–7 Importantly, drugs should not be withheld for fear of nephrotoxicity if they are essential to achieve early control of sepsis and IFI.8
The three cases presented highlight the effective use of liposomal amphotericin B in patients with IFIs and AKI in different clinical scenarios.
Case presentation
Case 1: fungal infection in a patient with advanced liver disease and AKI
Case presentation
A 63-year-old man presented to the accident and emergency department with haematemesis. At presentation, he was tachycardic and hypotensive, with clinical signs of ongoing bleeding and chronic liver disease, including ascites. Initial blood tests showed levels of haemoglobin at 73 g/L, platelets at 173×109 cells/L, sodium at 139 mmol/L and an international normalised ratio of 1.3. He was resuscitated with intravenous fluids and transferred to the intensive care unit (ICU) where he received further fluid resuscitation, including a two-unit blood transfusion. Urgent endoscopy under general anaesthesia revealed bleeding oesophageal varices which were treated by sclerotherapy and banding. He was ventilated with an endotracheal tube and received ongoing fluid support and blood transfusions. At day 3, he commenced prophylactic ciprofloxacin to provide antibiotic cover against bacterial infections of unknown type, including potential spontaneous bacterial peritonitis caused by his ascites. From admission to day 3, his serum creatinine increased from 80 µmol/L to 159 µmol/L, indicating AKI stage 2, consistent with his haemodynamic compromise in the setting of chronic liver disease. By day 7, the patient was showing clinical and haemodynamic improvements, but then developed a fever and became hypotensive. At this time, tests showed levels of haemoglobin at 94 g/L, platelets at 225×109 cells/L, sodium at 132 mmol/L, serum creatinine at 133 µmol/L and C-reactive protein (CRP) at 45 mg/dL. Prompt investigation of the cause of the fever was imperative, given the patient’s critically ill state.
Investigations
A sepsis screen of blood, urine and sputum samples was carried out, and blood cultures grew an unspecified fungus; subsequent plate culture and microscopy confirmed the presence of Aspergillus species. A transthoracic echocardiogram was normal, including an absence of heart valve lesions, and a CT scan of the chest did not indicate any typical changes consistent with aspergillosis, as shown in figure 1.
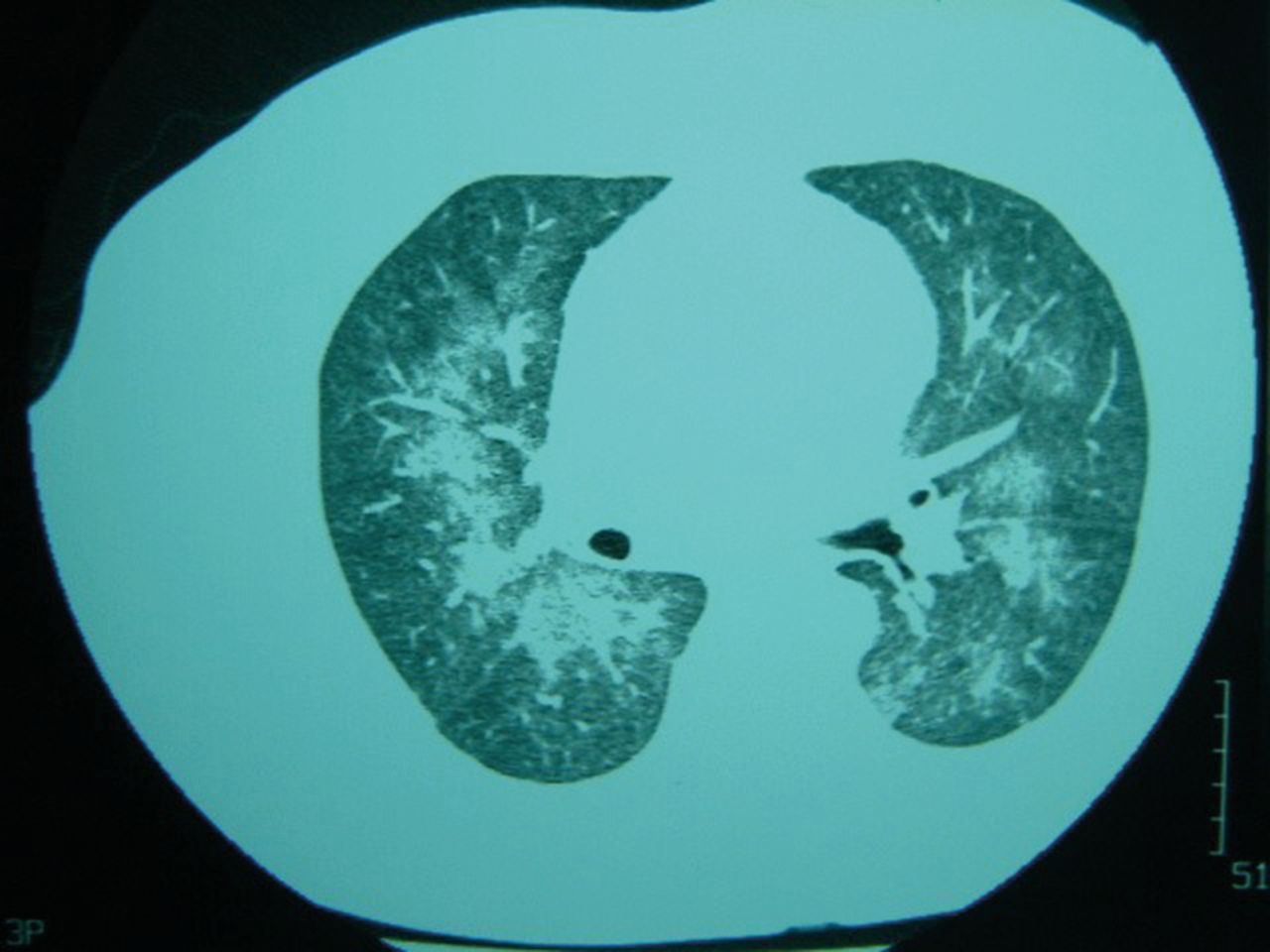
CT scan showing opacification indicative of early acute respiratory distress syndrome but no features of aspergillosis.
Differential diagnoses
At the time of the fever, the patient was initially diagnosed with sepsis of unknown cause. The differential diagnosis was wide, including hospital-acquired pneumonia, line infection, urinary tract infection, spontaneous bacterial peritonitis, endocarditis and pancreatitis. These possible diagnoses were excluded by carrying out organ-specific tests: urine cultures to rule out urinary tract infection, ascitic fluid cultures to rule out spontaneous bacterial peritonitis, blood tests and transthoracic echocardiogram to rule out endocarditis, amylase level tests to rule out pancreatitis, CT scan of the chest to rule out hospital-acquired pulmonary infection and renal ultrasound to exclude hydronephrosis.
Treatment
The fever was initially treated with broad-spectrum antibiotics (piperacillin/tazobactam and gentamicin), but the patient did not respond during 2 days of treatment. He developed worsening multiorgan failure, needing increasing vasopressor support and higher concentrations of oxygen to maintain adequate organ perfusion. Vancomycin was added empirically at day 9, and the central line changed in case it was the potential source of the infection. Following the growth of unspecified yeasts on day 10, liposomal amphotericin B at 3 mg/kg/day was added because of its broad spectrum of activity against a wide variety of fungal pathogens. The patient’s serum creatinine and CRP levels continued to rise and peaked at 273 µmol/L on day 13 and 455 mg/L on day 11, respectively, but thereafter improved. He had a normal urine output throughout this period.
Outcome and follow-up
On day 12, the patient’s vasopressor support started decreasing and his oxygen requirements decreased from 60% to 45%. When Aspergillus species were identified as the causative agent at day 13, it was elected that the patient should continue on liposomal amphotericin B. On day 16, he was weaned off vasopressor support. At day 33, he was discharged from the ICU. His serum creatinine returned to baseline levels and he was discharged home 2 weeks later. The level of kidney function change was consistent with the haemodynamic and septic status of the patient over the course of the illness. His continuing kidney function will depend on the status of his liver disease and future acute intercurrent illnesses. This patient will require ongoing, long-term monitoring of his kidney function.
Case 2: fungal infection in a patient with neutropenic sepsis and AKI
Case presentation
A 74-year-old man received an autologous stem cell transplant as part of treatment for mantle cell lymphoma. He had normal renal function prior to the transplant, but developed AKI stage 2 immediately post-transplant, with a serum creatinine level of 177 µmol/L. The cause of his AKI was thought to be multifactorial, but mainly due to severe vomiting and norovirus diarrhoea. An ultrasound scan of his urinary tract was found to be normal. His renal function recovered to baseline and he was discharged from hospital.
Six weeks later, he was readmitted to hospital with persistent vomiting and constipation. His serum creatinine was 84 µmol/L. A CT scan showed evidence of small bowel obstruction and an emergency laparotomy was performed to diagnose and relieve the obstruction. One week later, the patient developed a high spiking fever and pancytopenia, and his serum creatinine increased to 181 µmol/L, due to a combination of neutropenic sepsis and probable volume depletion. To provide antimicrobial cover prior to a confirmed microbiological diagnosis of the causative agent, the patient was treated with piperacillin/tazobactam and one dose of amikacin. Subsequent blood cultures grew Enterococcus faecium and vancomycin was added to the treatment regimen as a result. Vancomycin trough level measurements were performed regularly, and his renal function remained stable. A resection of the small bowel stenosis was sent for histological analysis.
Investigations
Histology on the small bowel tissue identified gastrointestinal mucormycosis with angioinvasion, as shown in figure 2.

Grocott methenamine silver stain of gastrointestinal lesion, showing mucormycosis in black.
Differential diagnoses
Differential diagnoses on presentation included localised infection, including tuberculosis (TB) and cytomegalovirus, and tumours. The subsequent CT showed small bowel obstruction but no mass; therefore, a tumour or mass effect secondary to specific infections, such as TB, was of low likelihood.
Treatment
The patient was initiated on liposomal amphotericin B at 5 mg/kg/day to treat the mucormycosis and received a 3-week course. Despite the concomitant use of one single dose of amikacin and a 2-week course of vancomycin, his renal function improved, with serum creatinine levels decreasing from 181 µmol/L to 80 µmol/L. During this period, there was a focus on optimal maintenance of haemodynamic and fluid status, and not using avoidable nephrotoxic agents. The patient maintained his urine output throughout as a result of aggressive hydration treatment.
Outcome and follow-up
The patient was discharged on oral posaconazole for 3 months for mucormycosis treatment. He remained well, with no further episodes of fungal infection. After 1 year in remission, he suffered a relapse of his mantle cell lymphoma and died 10 months later.
Case 3: fungal infection in an immunocompromised patient with AKI
Case presentation
A 32-year-old woman underwent a bilateral lung transplant for cystic fibrosis, and required long-term, daily maintenance immunosuppression including the calcineurin inhibitor tacrolimus. Thirteen months post-transplant, the patient presented in clinic with a productive cough and breathlessness, and a decrease in forced expiratory volume in 1 s (FEV1) from 2.35 L to 1.95 L; she was admitted to the ward. On admission, her serum creatinine level was normal at 75 µmol/L and she was taking prophylactic oral posaconazole (gastro-resistant tablets) due to a history of aspergillosis, and long-term isavuconazole (hard capsules) due to previous Fusarium infection. A drop in FEV1, combined with clinical symptoms, mandated further investigation.
Investigations
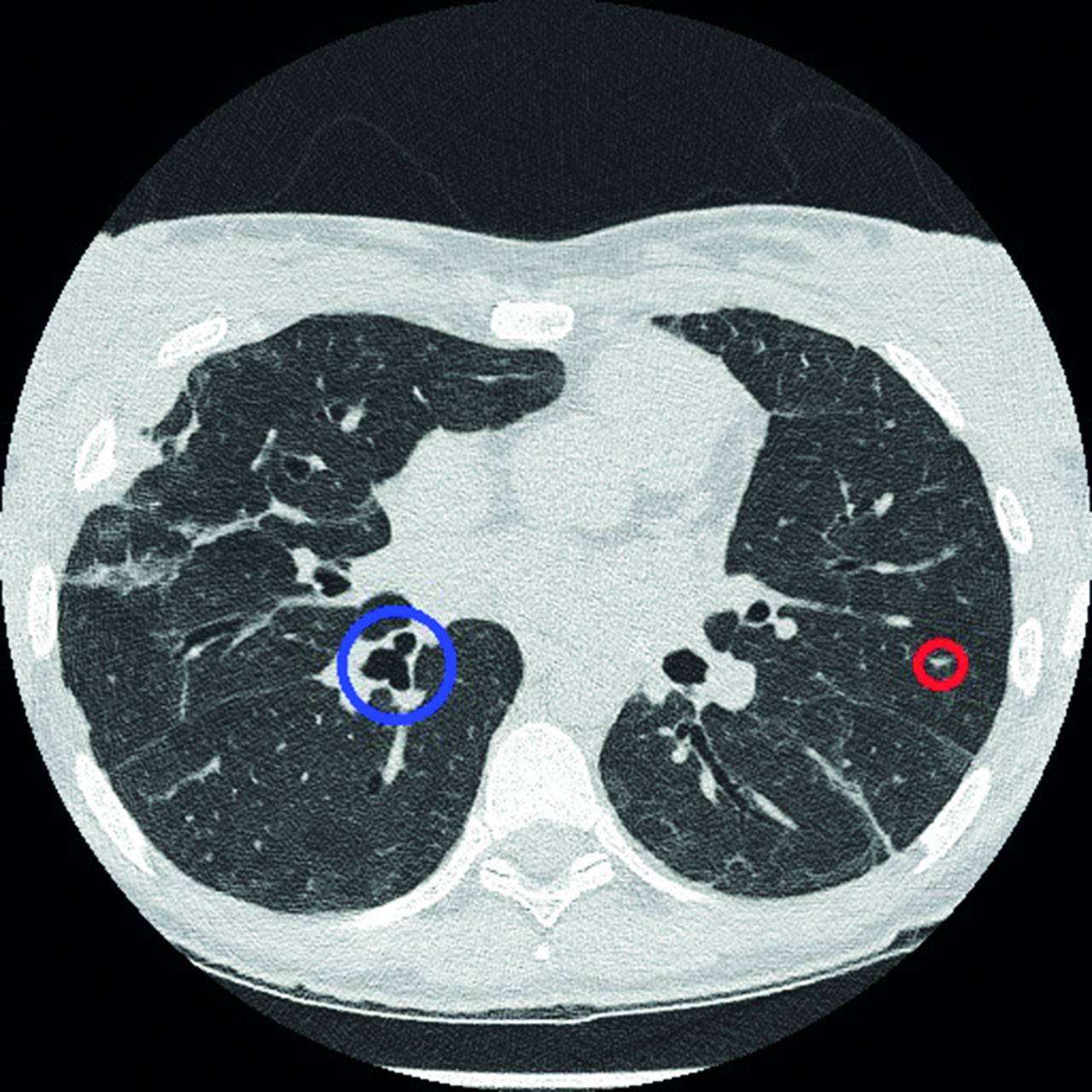
A CT scan was performed, which indicated chest abnormalities, as shown in figure 3. A bronchoscopy was carried out and culture of bronchoalveolar lavage fluid showed the presence of Fusarium and Elizabethkingia miricola.

{kind=link}
{kind=link}
{kind=link}
CT scan showing nodules (circled in red) and airway thickening (circled in blue).
Differential diagnoses
As the patient presented with a productive cough, a bacterial or fungal infection was suspected and further investigated using bronchoscopy. Histology obtained during the bronchoscopy showed interstitial changes with no evidence of obliterative bronchiolitis, suggesting that acute rejection of the lung transplant was unlikely. Reverse-transcriptase PCR (RT-PCR) was used to investigate a panel of 14 respiratory viruses, including coronavirus OC43 infection, and nasopharyngeal aspirates (NPA) were collected to test for infection with respiratory syncytial virus (RSV).
Treatment
On admission (day 0), the patient was immediately started on broad-spectrum antibiotics (piperacillin/tazobactam and tigecycline) to provide cover for suspected bacterial infections of unknown type. RT-PCR was negative for all 14 respiratory viruses, but NPA testing confirmed the presence of RSV; this was treated with methylprednisolone and ribavirin. On day 1, liposomal amphotericin B at 3 mg/kg/day was started as treatment for Fusarium and the isavuconazole dosage was increased. She was discharged from hospital on day 13 but, due to progressive respiratory decline, continued to receive liposomal amphotericin B at home, through a peripherally inserted central catheter. Her serum creatinine level rose throughout this period, peaking at 186 µmol/L on day 26, but this was managed by excluding obstruction, and optimising fluid and haemodynamic status.
Outcome and follow-up
A bronchoscopy was performed on day 27, which was reported as culture-negative. The patient remained well, with no further episodes of fungal infection, and her renal function recovered to normal levels, with no lasting impairment.
Discussion
The Kidney Disease: Improving Global Outcomes guidelines recommend that exposure to nephrotoxic drugs should be limited in patients with or at risk of developing AKI, and that a risk/benefit assessment is carried out to weigh the risk of developing or worsening the AKI against the risk associated with not using the agent.1
IFIs are a major cause of death in critically ill patients, particularly in the setting of immunosuppression, such as following bone marrow transplantation or solid organ transplantation.2 AKI in these patients is very common and can be associated with both sepsis itself and complications arising from its treatment.9 In this clinical setting, it can be difficult to quantify the contribution of individual components to a patient’s AKI. A careful assessment of the potential risk of a medication in the setting of AKI is essential. Paradoxically, in a critically ill patient, this may be a straightforward decision; if there is significant likelihood of an IFI, the patient will die without prompt treatment; therefore, commencement of antifungal therapy is essential. In all three cases reported here, prompt and efficient treatment of the IFI was critical to the survival of the patient and, therefore, the use of liposomal amphotericin B was deemed necessary. None of the patients experienced any lasting kidney damage as a result of this decision.
There are two specific clinical scenarios where the use of liposomal amphotericin B should be considered. First, where there is uncertainty around the species of the fungal agent in a critically ill patient and second, where the fungus is susceptible to amphotericin B.
Delays between the clinical diagnosis of a likely IFI and confirmation of that diagnosis are common. Therefore, empirical treatment with liposomal amphotericin B may be indicated, as this will provide broad-spectrum antifungal treatment against candidiasis, aspergillosis and mucormycosis, which can be resistant to other antifungals, such as certain azoles.10–12 It is important to continue to pursue a specific diagnosis after institution of liposomal amphotericin B. For example, if aspergillosis is subsequently confirmed, and there is a clear clinical requirement, then consideration may be given to switching to an alternative agent with narrow-spectrum efficacy and a lower incidence of renal complications than liposomal amphotericin B.
There is a long-standing recognition of the high risk of AKI in patients treated with conventional amphotericin B. In a large retrospective analysis carried out in 494 adult inpatients, 28% developed nephrotoxicity, defined as either a ≥50% increase from baseline or doubling of serum creatinine levels.13 Liposomal amphotericin B is substantially less nephrotoxic than conventional amphotericin B; a meta-analysis reported nephrotoxicity incidence rates of 14.5% and 32.5%, respectively.14 These differences in nephrotoxicity may reflect both the distribution and structure of the drugs; for example, liposomal amphotericin B does not contain deoxycholate, which can cause direct renal tubular toxicity.15 Additionally, liposomal amphotericin B has been successfully used to treat IFIs in critically ill patients with impaired renal function at treatment initiation without adverse impact on renal function, as measured by serum creatinine levels.16 17
Patients with AKI who are receiving liposomal amphotericin B, or indeed any other drug with a potential effect on renal tubular function, should receive high-quality supportive care to maintain or restore the function of the distal tubular cells of the kidney. Optimal management of fluid balance and electrolytes and acid–base status is required. All electrolytes that are regulated by the renal tubules should be monitored and replaced if below the normal range. It is important to replace all depleted electrolytes as, for example, replacement of potassium in a patient who is hypomagnesaemic and/or hypophosphataemic (or vice versa) without replacing magnesium and/or phosphate will not help the underlying tubular deficit. Metabolic acidosis can be corrected through the administration of bicarbonate, which is best given as an isotonic solution. With accurate monitoring and supplementation, the majority of patients should be able to continue on their course of liposomal amphotericin B.
While there are several, recently published cases describing the successful use of liposomal amphotericin B in the treatment of various IFIs,18–20 to our knowledge, this is the first case series to specifically examine its use in patients with AKI. Each case illustrates a clinical course of improvement and recovery while the patient was on treatment with liposomal amphotericin B. In our experience, AKI is a frequent consideration in prescribing of antifungal agents in the critically ill patient. These cases therefore allow us to explore the decision-making processes for the use of antifungal agents in this setting. We believe that there are clear signposts on how to use liposomal amphotericin B in the setting of AKI. These comprise:
Ensuring that the presence of an IFI is considered in all critically ill patients.
If a patient commences treatment on clinical grounds alone, tests to establish a diagnosis of the agent causing the IFI should continue.
AKI is not a contraindication to commencing treatment with liposomal amphotericin B where there is a clinical diagnosis of a potential life-threatening IFI.
A discussion around the risk/benefit of starting liposomal amphotericin B should take place both within the clinical team and with the patient and/or their next of kin. This discussion should be carefully documented.
The patient should receive appropriate supportive care to optimise their kidney function, which should be monitored daily.
Further formal risk/benefit assessments should be carried out in the event of:
worsening AKI.
microbiological confirmation of the causative agent.
In conclusion, while there is no published literature to provide evidence for practice, AKI and IFI are common in critically ill patients. Our case studies indicate that the use of liposomal amphotericin B to treat IFIs in critically ill patients with AKI may be indicated where the fungal species is unknown or where susceptibility to amphotericin B is known. With prompt treatment with liposomal amphotericin B, alongside high-quality supportive care, good clinical outcomes can be achieved.
Learning points
Acute kidney injury (AKI) and invasive fungal infections (IFIs) are common in critically sick patients, and both should be key considerations during the management of such patients.
Prompt treatment of the IFI is critical to patient survival.
A careful, documented assessment of the potential risk of a medication in the setting of AKI is essential.
Liposomal amphotericin B to treat IFIs in critically sick patients with AKI may be indicated where the fungal species is unknown or where susceptibility to amphotericin B is known.
It is important to continue to pursue a specific diagnosis after the institution of liposomal amphotericin B.
Acknowledgments
The authors would like to thank Dr Sarah Bryant of Axiom Health Ltd. for medical writing and editorial support, which was funded by Gilead Sciences Ltd.
References
Footnotes
Contributors PC conceived the manuscript. DA-J, MK and MO were responsible for acquisition of the data and obtaining patient consent. All authors were responsible for analysis and interpretation of the data, revising the article critically for important intellectual content, and final approval of the version to be published.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests DA-J reports personal fees from Gilead, during the conduct of the study; other from Pulmocide Ltd, outside the submitted work. PC reports personal fees from Gilead, during the conduct of the study.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.