Article Text

Statistics from Altmetric.com
Description
A 59-year-old man with a history of chronic obstructive pulmonary disease (COPD) presented with progressive dyspnoea and bilateral leg swelling over 3–4 weeks. He had dyspnoea on moderate exertion at the baseline but progressed to symptoms at rest along with new onset of orthopnoea. He reported no chest pain, palpitations, syncope, fever, chills, wheezing or productive cough. His mother and brother died at ages 54 and 44, respectively, after developing heart failure of unknown aetiology. He has a smoking history of 40 pack-year. His physical examination on admission revealed stable vitals, elevated jugular venous pulse (JVP), normal S1 and S2 sounds, regular heart rate, no murmur, rubs or gallop, diminished breath sounds in bilateral bases with occasional wheezing and bibasilar rales. His lower extremities revealed bilateral 1+ non-tender pitting oedema with clubbing.
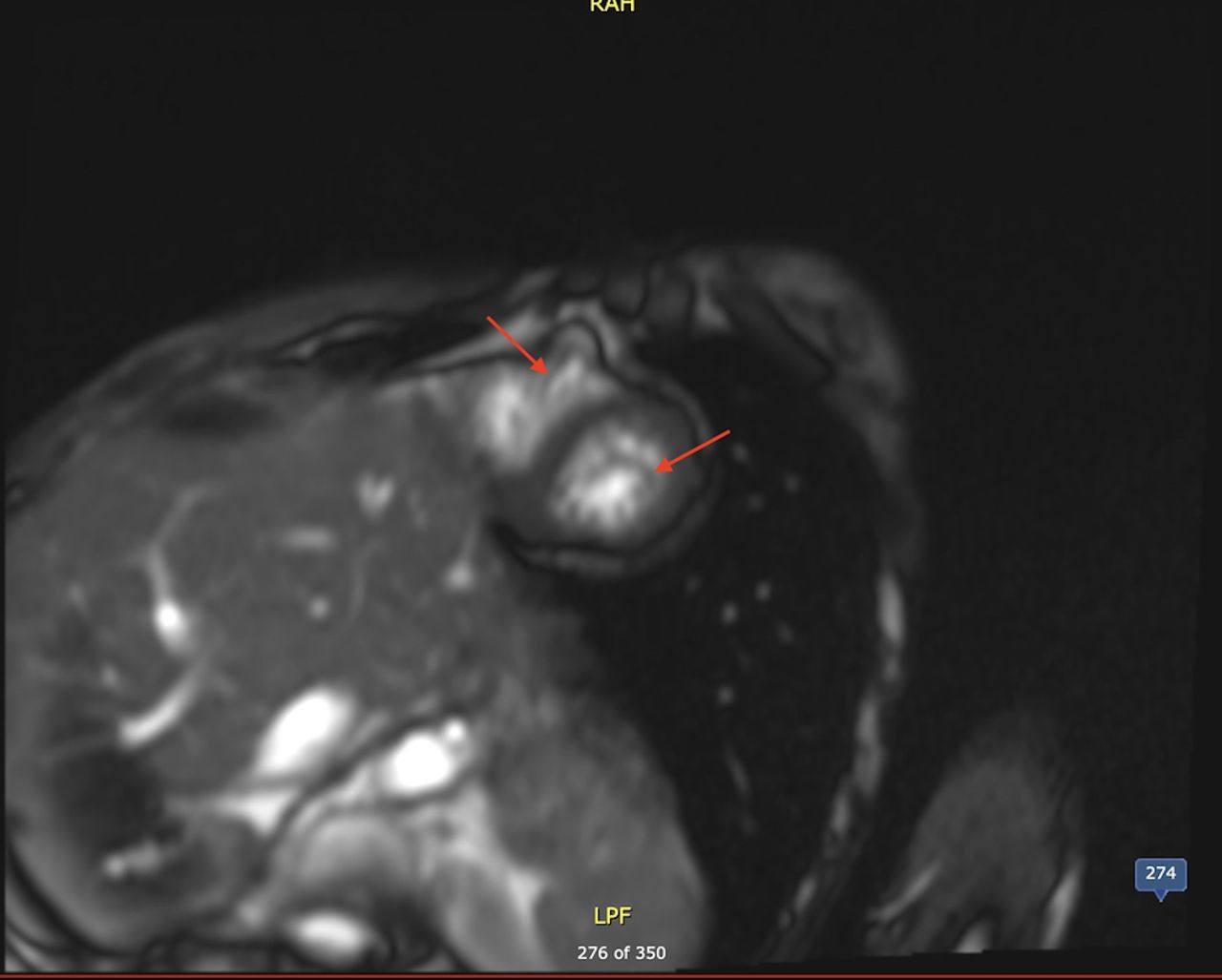
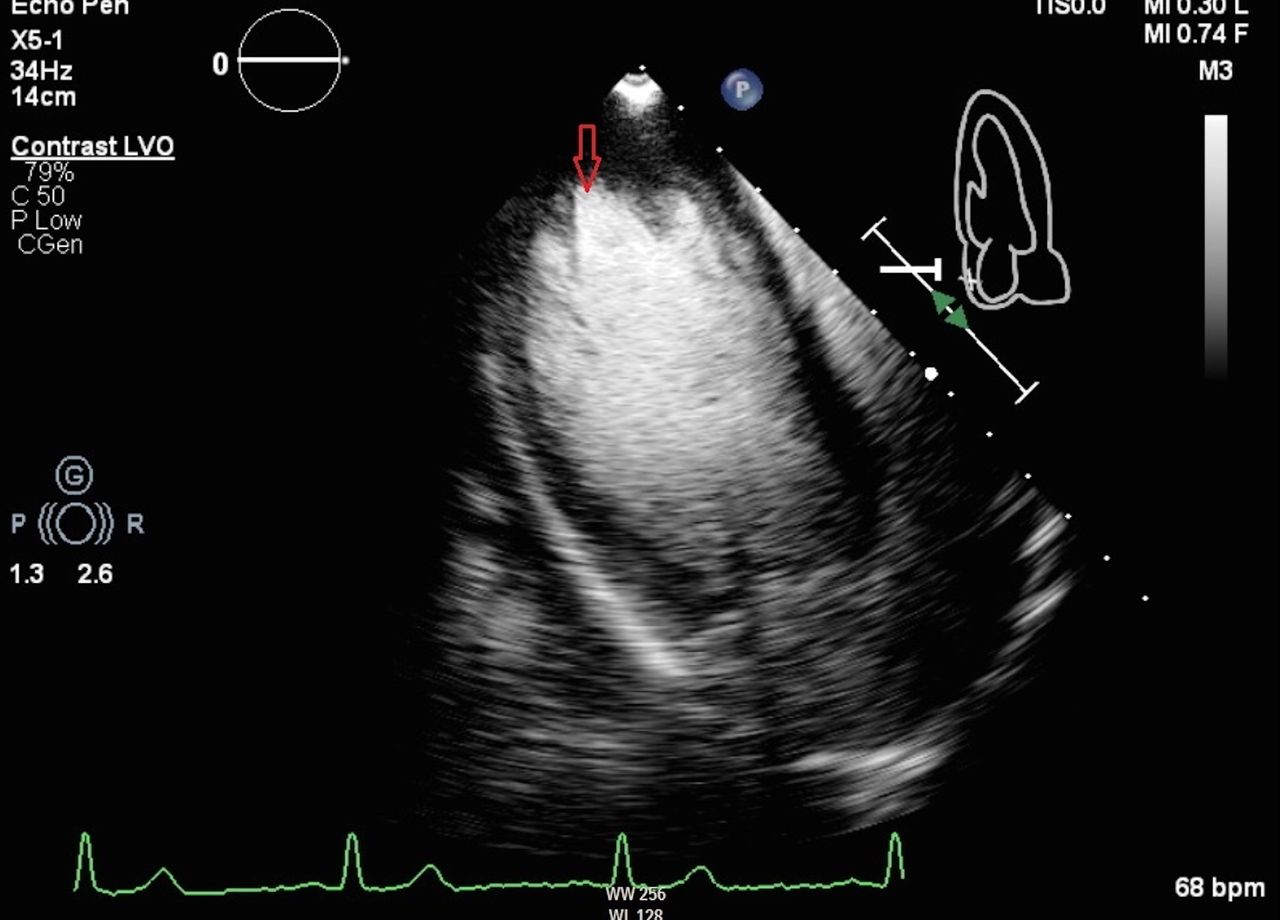
The electrocardiogram showed sinus tachycardia with a right axis deviation with evidence of left ventricular hypertrophy and right atrial enlargement. There were no ischaemic changes. Chest X-ray (CXR) was normal. An echocardiogram showed global hypokinesia with a left ventricular ejection fraction of 35%–40% with grade I diastolic dysfunction and probable non-compaction of the left ventricle (figures 1 and 2). Right ventricular function and right ventricular systolic pressure were normal. A provisional diagnosis of left ventricular non-compaction (LVNC) was made. He was started on furosemide, lisinopril and carvedilol. Bilateral cardiac catheterisation showed normal coronary arteries with elevated pulmonary wedge pressure consistent with non-ischaemic cardiomyopathy. Cardiac MRI confirmed increased trabeculation in both ventricular apices with impaired biventricular systolic function confirming biventricular non-compaction (BVNC) cardiomyopathy (figures 3–5).

An echocardiogram with contrast shows intertrabecular crevices filled with contrast (red arrow).

An echocardiogram shows left ventricular non-compaction (red arrow).

A cardiac MRI shows bi-ventricular non-compaction (red arrows). LPF: low pass filter.

A cardiac MRI with contrast—end-diastolic view showing biventricular non-compaction (red arrows). LPF: low pass filter.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
A cardiac MRI with contrast—end-systolic view showing biventricular non-compaction (red arrows). LPF: low pass filter.
Non-compaction is thought to be due to intrauterine arrest of compaction of the loose interwoven meshwork present in fetal myocardial primordium.1 2 Alternatively, the pronounced hypertrabeculation may be due to altered regulation in cell proliferation, differentiation and maturation during ventricular wall formation.1 2 Clinically, it may have variable manifestations of heart failure, chest pain, thromboembolic events, atrial and ventricular arrhythmias and risk of sudden cardiac arrest.1 2 It is recommended to undergo Holter monitoring to screen for arrhythmias as there is a role of an implantable cardioverter-defibrillator (ICD).1 Oral anticoagulation is recommended if there is arrhythmia, atrial or ventricular thrombi or for primary prevention of thrombus in case of left ventricular (LV) dysfunction.1 Our patient presented with new-onset heart failure with biventricular systolic dysfunction, and non-obstructive coronary artery disease (CAD) on cardiac catheterisation suggesting BVNC to be aetiology of heart failure. There have been very few cases of patients with BVNC reported, presenting as heart failure, tonic-clonic seizure.3–5 Holter monitor did not reveal any arrhythmias and he did not meet criteria for ICD placement or anticoagulation. A recent follow-up cardiac MRI showed persistent BVNC but normalisation of LV systolic dysfunction with optimal guideline-directed medical therapy for cardiomyopathy. Genetic counselling was advised as it can be familial. He chose not to be evaluated as he improved symptomatically with medical therapy and continues to be in the follow-up. In our patient, we can speculate that the family history of heart failure of unknown aetiology was likely due to non-compaction cardiomyopathy.
Learning points
Isolated ventricular non-compaction can be sporadic or familial and is characterised by prominent trabeculae and deep intertrabecular recesses. Left ventricular non-compaction (LVNC) has been found in 0.014%–1.3% of patients undergoing echocardiography (biventricular non-compaction being even rarer), and it is an uncommon cause of heart failure and sudden cardiac death.
Echocardiography is used both to establish the diagnosis of non-compaction cardiomyopathy and as an aid during follow-up. Jenni et al proposed the following three criteria for diagnosis6: (1) a thickened left ventricular wall composed of two layers: a thin compacted epicardial layer and a non-compacted endocardial layer with numerous prominent trabeculations and deep recesses: a maximum ratio of non-compacted to compacted myocardium being >2:1 at end systole in the parasternal short-axis view, (2) colour Doppler evidence of flow within the deep intertrabecular recesses and (3) prominent trabecular meshwork in the left ventricular (LV) apex or midventricular segments of the inferior and lateral wall.
Cardiac MRI (CMR) criteria for LVNC are still evolving. The following end-diastolic and end-systolic CMR criteria have been proposed as per various studies conducted so far. (1) A maximum end-diastolic non-compacted to compacted myocardial thickness ratio of >2.3 was the best criterion for LVNC and yielded a sensitivity of 86% and specificity of 99% for LVNC. (2) A trabeculated LV mass > 20% of global LV mass was identified as a criterion for LVNC with a sensitivity of 94% and a specificity of 94%. (3) Fractal dimension as a quantitative measure of trabeculation is high in LVNC and may be very accurate; however, further follow-up is needed to better identify its role. (4) An end-systolic non-compacted to compacted (thickness) ratio ≥ 2.0 was found to be more strongly associated with heart failure and with adverse events (heart failure, death, heart failure readmission, embolic events and ventricular arrhythmias) than other criteria for LVNC.
Footnotes
Presented at This case has been presented as a poster in ACP, MA, 2018
Contributors MPS: writing, editing and critical review of the manuscript. AD: retrieval of images and critical review of the manuscript. DP: critical review and editing of the manuscript. YK: retrieval of images and editing of manuscript. RH: inception of the idea and critical review of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.